
Vitrectomy is an eye surgery that involves removing the transparent gel called the vitreous, located in the center of the eye. It is performed to treat certain retinal diseases that may threaten vision. Dr Julien Gozlan, ophthalmic surgeon in Paris 16, explains the principle of this surgery, its main indications, and how the procedure is carried out.
What is vitrectomy?
Inside the eye, behind the lens, there is a large cavity filled with a transparent gel: the vitreous. This gel is not essential for vision. During a vitrectomy, the surgeon removes this vitreous and replaces it with a clear fluid or sometimes with a gas or silicone oil.
The purpose of vitrectomy is not to "clean" the eye cosmetically, but to treat a retinal disease or a complication that impairs or threatens vision: vitreous hemorrhage, retinal tear or retinal detachment, membrane on the surface of the macula, macular hole, etc.
Vitrectomy is performed in a specialized operating room, under local or general anesthesia, with the aid of an operating microscope. The patient lies on their back throughout the entire procedure.
When is vitrectomy recommended?
Vitrectomy is indicated when the vitreous or the retina is causing significant visual impairment or poses a risk to vision. The main indications include:
- Vitreous hemorrhage: blood fills the vitreous and blocks light, causing vision to become very blurry or dark.
- Retinal detachment: the retina separates from its underlying support, which can lead to permanent vision loss without prompt surgery.
- Epiretinal membrane: a thin film forms on the surface of the macula and "wrinkles" it, distorting images.
- Macular hole: a small hole forms at the center of the retina, causing decreased central vision.
- Complicated diabetic retinopathy
- High myopia with macular involvement (foveoschisis, vitreomacular traction).
- Severely debilitating floaters, in certain carefully selected cases.
In some situations, vitrectomy is the first step, and then other treatments are performed during the same procedure: retinal endolaser, cryotherapy, membrane peeling, gas injection, or silicone oil injection.
How is a vitrectomy performed?
Before the procedure
A complete ophthalmological work-up is performed before surgery: retinal examination, OCT, and sometimes angiography or ocular ultrasound. The type of anaesthesia (local or general) is discussed with the surgeon and anaesthetist according to your health status and the expected duration of the procedure.
Anaesthesia and preparation in the operating theatre
Anaesthesia is most often local peribulbar (injection around the eye to numb and immobilise the globe) or general in some cases. A sterile drape is applied and the surgeon operates under an operating microscope.
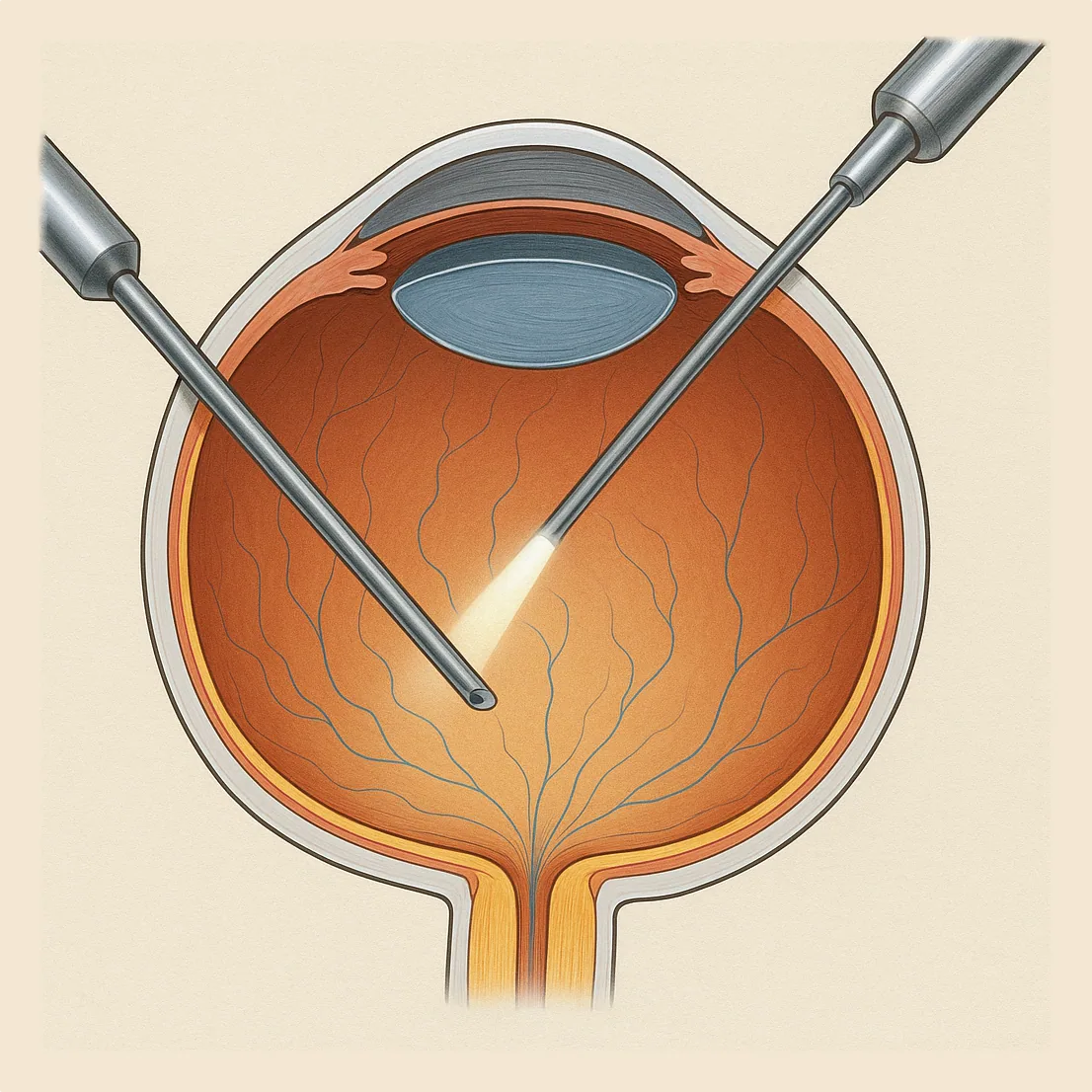
Placement of trocars
Three micro-incisions of less than 1 mm are made in the sclera (white part of the eye). Trocars are inserted to serve as entry ports for the instruments. One is connected to a continuous infusion of sterile saline to maintain intraocular pressure and volume throughout the procedure.
Central vitrectomy
The surgeon introduces the vitrector (cutting-aspiration probe) and an endoilluminator through the trocars. Central vitreous gel is progressively removed under direct microscope visualisation, working from the centre of the cavity outward.
Peripheral vitrectomy
To reach the vitreous base (peripheral attachment zone), an assistant applies scleral indentation — gentle external depression of the eye wall — bringing the peripheral retina into view. Peripheral vitreous is removed and the entire retinal periphery is examined.
Treatment of the underlying cause
Depending on the condition, one or more additional procedures are performed:
- Membrane peeling (epiretinal or internal limiting membrane): removed with microsurgical forceps, often aided by a vital dye (brilliant blue, triamcinolone);
- Endolaser photocoagulation: laser treatment of retinal tears or barrier laser around a detachment;
- Cryotherapy: application of cold via an external probe to peripheral tears inaccessible to the laser;
- Retinotomy/retinectomy: incision or resection of rigid retina caused by proliferative vitreoretinopathy (PVR) to allow flattening;
- Internal tamponade: injection of gas (SF6, C3F8) or silicone oil to hold the retina in place during healing.
Tamponade and closure
At the end of surgery, the vitreous cavity is filled with clear saline, gas, or silicone oil as appropriate. The micro-incisions are self-sealing in most cases and require no sutures. An eye pad is applied.
Postoperative course and recovery
After vitrectomy, the eye may be red, sensitive, or slightly painful for a few days. Antibiotic and anti-inflammatory eye drops are prescribed for several weeks.
If an intraocular gas was used, vision is often very blurry at first: you may see a large black bubble or a horizontal line moving in your field of vision. The gas gradually resorbs over a few days to several weeks.
In some cases, you may be asked to maintain a specific head position (face down into a pillow or on your side) for several hours a day, so that the gas presses against the area being treated (for example, in the case of a macular hole).
Resumption of activities depends on the procedure performed and visual recovery. Driving, contact sports, and heavy lifting are generally not recommended for a certain period of time. The surgeon will provide you with personalized instructions based on your individual situation.
Risks and possible complications
As with any surgery, vitrectomy carries risks, although they remain rare relative to the expected benefit. The main possible complications include:
- Intraocular infection (endophthalmitis), exceptional but serious.
- Intraocular hemorrhage.
- Retinal detachment after the procedure.
- Increased intraocular pressure.
- Accelerated cataract development in patients who have not yet undergone cataract surgery.
Your surgeon will explain these risks in detail before the operation and will verify that the expected benefit for your vision justifies performing the vitrectomy.
When should you consult Dr Julien Gozlan?
If you experience a sudden or gradual loss of vision, sudden floaters, flashes of light, a dark spot in your visual field, or if you have been told about a retinal disease that may require surgery, it is important to consult a specialized ophthalmologist.
FAQ: frequently asked questions about vitrectomy
How long does a vitrectomy take on average?
The duration of a vitrectomy depends on the procedure to be performed on the retina, but most surgeries take between 30 minutes and 1 hour 30 minutes. A straightforward case (isolated vitreous hemorrhage, small macular hole) is generally quicker than a complex retinal detachment or advanced diabetic retinopathy. In addition to the surgical time, there is the preparation time in the operating room and monitoring in the recovery room.
Is vitrectomy painful during or after the procedure?
During surgery, the eye is anesthetized (local or general anesthesia) and you should not feel any pain, only a sensation of pressure or contact. After vitrectomy, the eye may be sensitive, red, or slightly painful for a few days: eye drops and sometimes mild analgesics are generally sufficient to manage this discomfort. However, significant or worsening pain should be reported to the surgeon promptly.
How long does the gas remain in the eye after vitrectomy?
The duration the gas remains depends on the type and concentration of gas used. Depending on the case, it may resorb within one to two weeks, or persist for several weeks. During this period, vision is blurry and you often see a moving bubble in your field of vision. The gas gradually disappears, replaced by the eye's natural fluid, without the need for surgical removal.
Can you fly or go to high altitude after vitrectomy with gas?
As long as gas remains in the eye, flying or traveling to high altitude is strictly prohibited. The decrease in atmospheric pressure can cause the bubble to expand, leading to severe pain and elevated intraocular pressure that could result in blindness. Your surgeon will tell you precisely when the gas has completely resorbed and when air travel or mountain trips can safely resume.
Will cataract surgery be needed after vitrectomy?
Vitrectomy often accelerates the development of a cataract in patients who still have their natural lens, especially after the age of 50. This does not mean the cataract appears immediately, but it may progress more quickly in the months or years following surgery. If it becomes bothersome for vision, cataract surgery can be offered at a later time. In some cases, vitrectomy and cataract surgery can even be performed during the same procedure.
How soon can you return to work and resume driving?
Returning to work and driving depends on the surgery performed, whether gas was used, and your type of professional activity. For office work, time off ranging from a few days to a few weeks is common. Driving is only permitted once vision is sufficiently clear and stable, and the visual field allows safe driving. These timelines are therefore assessed on a case-by-case basis during follow-up appointments with your surgeon.
Are there specific precautions for sleeping or exercising after vitrectomy?
After surgery, certain positions may be recommended (for example, sleeping on one side or in a face-down position) when gas has been injected to treat a macular hole or retinal detachment: these instructions are personalized and limited in duration. Regarding exercise, gentle activities (walking, stationary cycling) are generally resumed first, while contact sports, ball sports, or activities with a risk of impact to the head are postponed for several weeks. Again, the timeline is tailored to your clinical situation and the progression of retinal healing.
Dr Julien Gozlan, ophthalmologist in Paris 16, specializes in retinal and cataract surgery. He welcomes you for a comprehensive assessment, explains the various treatment options, and, if necessary, the details of a vitrectomy.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan welcomes you at Paris – Auteuil Ophthalmology Practice for the diagnosis and management of retinal diseases and the possible performance of a vitrectomy.
Book an AppointmentFurther reading
- OCT: an imaging examination to analyze the retina.
- Retinal detachment: symptoms, emergency, and treatments.
- Epiretinal membrane: when should vitrectomy be considered?
- Macular hole: causes and surgical management.
- Retinal emergencies treated by vitrectomy : retinal detachment and other emergencies requiring rapid intervention.