
Myopic foveoschisis is a degenerative macular condition specific to high myopia, characterized by progressive splitting of the retinal layers at the fovea. Long underdiagnosed, this condition is now identified thanks to optical coherence tomography (OCT). Dr Julien Gozlan, ophthalmic surgeon specializing in vitreoretinal surgery at the Paris – Auteuil Ophthalmology Practice, provides a comprehensive overview of this disease: definition, pathophysiological mechanisms, symptoms, imaging diagnosis, surgical indications, operative techniques, and visual prognosis.
What is myopic foveoschisis?
Myopic foveoschisis, also known as high myopia foveoschisis, corresponds to the development of cystic cavities within the neuroretinal layers in the macular region. First described in 1938 by Rochon-Duvigneaud, this macular retinoschisis long went unrecognized because it was difficult to detect on simple fundus examination. It was in 1999 that Takano and Kishi, thanks to the advent of OCT, refined its definition by characterizing it as an intraretinal splitting that may be associated with photoreceptor detachment.
Myopic foveoschisis occurs in patients with high myopia (axial length generally greater than 26 mm), most often in the presence of a posterior staphyloma. Its incidence ranges from 8 to 34% depending on published series, and it affects 9 to 20% of myopic eyes with a staphyloma. There is a female predominance. An essential point: the discovery of myopic foveoschisis does not necessarily imply decreased vision, and many cases are identified incidentally during a routine OCT examination.
Pathophysiology of myopic foveoschisis: complex mechanical forces
Understanding myopic foveoschisis relies on identifying biomechanical and degenerative forces that progressively stretch and dissociate the retinal layers. Three types of traction can be schematically distinguished:
Tangential traction (passive)
- Epiretinal membranes: present in approximately 30% of myopic foveoschisis cases, epiretinal membranes exert a tractional force on the macula, contributing to retinal splitting.
- Internal limiting membrane (ILM) rigidity: the proliferation of collagen fibers and cellular debris on the ILM surface causes it to stiffen. On OCT, this rigidity manifests as detachment of the ILM from the deeper retinal layers.
- Vascular component: retinal arterioles that have become rigid create horizontal microfolds visible on OCT, giving an appearance of retina stretched between two vascular anchoring points.
Anteroposterior centrifugal traction (passive)
The posterior staphyloma and progressive scleral elongation constitute a centrifugal force that carries the outer retina backward. This posterior ectasia gradually increases with age and axial length of the globe. The development of a staphyloma, typically around age 40, significantly increases mechanical stress on the retina, inducing changes at the vitreomacular interface that lead to the development of schisis, or even progression to a macular hole.
Anteroposterior centripetal traction (active)
Vitreomacular adhesions exert active forward traction. In highly myopic patients, the posterior hyaloid is often highly adherent, and the persistence of posterior vitreous cortex remnants is frequently observed during vitrectomy. Contraction of this vitreous cortex displaces the retina anteriorly, while the presence of an epiretinal membrane reinforces vitreomacular adhesion and opposes spontaneous vitreous detachment.
All of these intertwined mechanisms — tangential, centrifugal, and centripetal traction — oppose the adaptation of the retina to the curvature of the staphyloma and contribute to the progressive development of myopic foveoschisis, with a risk of progression to a full-thickness macular hole.
Symptoms and diagnosis of myopic foveoschisis
Functional signs
Myopic foveoschisis can be completely asymptomatic, particularly when pre-existing myopic chorioretinal degeneration already limits visual function. When symptomatic, the patient most often reports:
- A progressive decrease in visual acuity over several months or even years.
- Metamorphopsia (distortion of straight lines), the date of onset of which is often difficult to specify.
- Reading becoming more "tiring," with a progressive loss of enjoyment in reading.
More rarely, the reason for consultation is an inaugural complication: sudden central scotoma due to the development of a macular hole or retinal detachment of the posterior pole.
Central role of OCT in diagnosis
The diagnosis of myopic foveoschisis relies essentially on OCT, which is the most sensitive and specific tool. Fundus examination alone is often insufficient due to the deformation caused by the staphyloma and the media opacities frequently found in highly myopic patients.
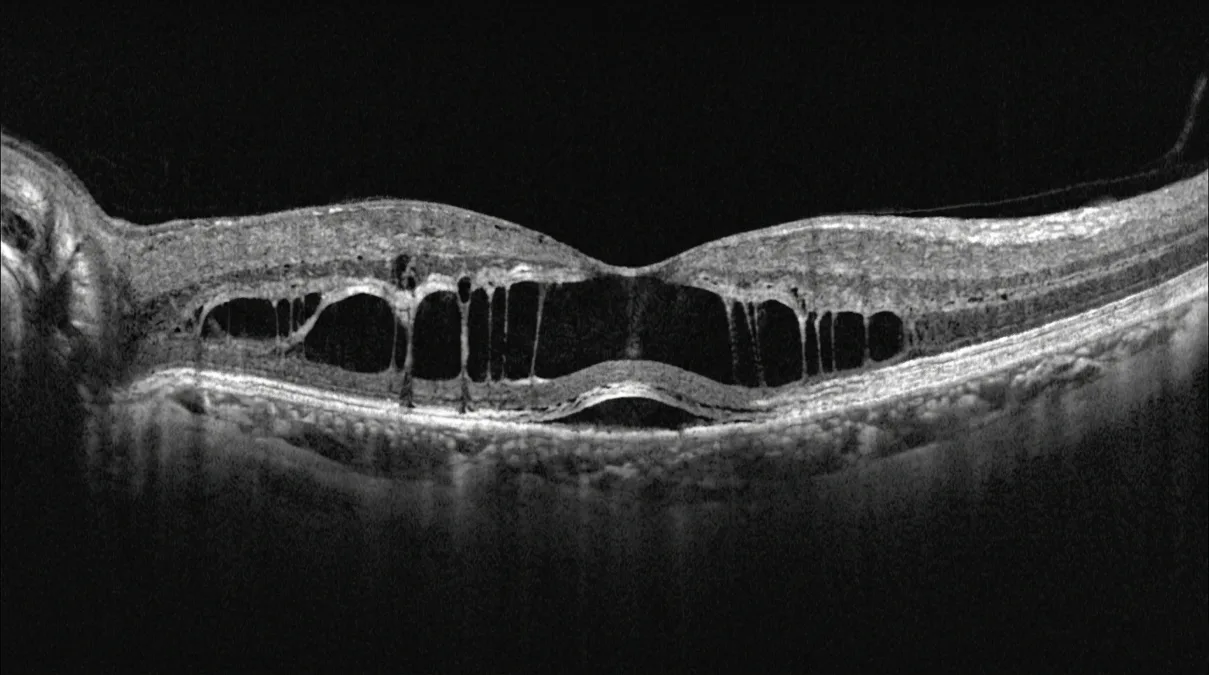
On OCT, myopic foveoschisis presents as a thickened retina in the macular region, with splitting between the outer retina (thin, hyporeflective) and the inner retina (thick, hyperreflective). Tissue columns, likely corresponding to residual Müller cells, connect the two layers. Swept-source OCT and OCT angiography allow better visualization of retinochoroidal structures, vitreoschisis, and peripheral schisis.
Several evolutionary stages are identified:
- Pure retinoschisis: splitting within the outer nuclear and outer plexiform layers, with modest functional impact (visual acuity often between 20/30 and 20/60).
- Foveolar neuroepithelial detachment: the stage at which a significant decrease in visual acuity is perceived by the patient.
- Macular hole and/or retinal detachment: advanced stages, most often requiring surgical management.
The cotton ball sign, described by Tsunoda et al., corresponds to a round hyperreflective zone at the center of the fovea on SD-OCT, between the ellipsoid line and the photoreceptor tips. It constitutes an early sign of outer retinal damage.
Surgical treatment of myopic foveoschisis
Surgical indications
Treatment of myopic foveoschisis is never an emergency (except in the case of extensive retinal detachment). The retina of the highly myopic eye appears paradoxically capable of tolerating tractional forces that would be intolerable in a non-myopic patient. Surgical indication is established when there is:
- Documented functional deterioration over several months (decrease in visual acuity making reading difficult with an age-appropriate addition).
- Major anatomical worsening on OCT: increase in schisis height, development of foveolar detachment, macular hole, or retinal detachment.
- The association of myopic foveoschisis with a retrofoveolar serous detachment, prompting surgery before the development of a full-thickness macular hole.
Vitrectomy: the reference technique
The treatment of choice for myopic foveoschisis is vitrectomy, which aims to relieve all tractional forces exerted on the macula. The procedure includes several operative steps:
- Posterior hyaloid detachment: performed completely and carefully. Vitreous cortex residues are identified using triamcinolone acetonide and removed by tangential traction.
- Dissection of epiretinal membranes if present.
- Internal limiting membrane (ILM) peeling: a subject of debate. Some authors recommend peeling over two to three disc diameters within the vascular arcades, facilitated by Coomassie blue (Brilliant Blue G). Others propose fovea-sparing peeling to limit the risk of iatrogenic macular hole.
- Gas tamponade: discussed on a case-by-case basis, indicated when a macular hole is present but not essential for the reattachment of isolated myopic foveoschisis.
In cases of large-diameter macular holes (greater than 400 µm), the use of an ILM flap technique achieves closure rates reaching 98%. In patients with axial lengths exceeding 33 mm, extended-length surgical instruments are sometimes essential to access the posterior pole.
Other surgical options
Combined phacoemulsification/vitrectomy surgery: when nuclear lens opacification limits intraoperative visualization, combined cataract surgery is systematically performed, although it raises the issue of anisometropia in a patient who is often still young and phakic in the fellow eye.
Macular buckling: proposed as an alternative or complement, this technique reverses the curvature of the staphyloma and allows treatment of foveolar detachments associated with myopic foveoschisis, without requiring posterior sutures on a thinned sclera.
Prognosis and outcomes of surgically treated myopic foveoschisis
The natural course of myopic foveoschisis, in the absence of treatment, is often unfavorable: a decrease in visual acuity is observed in 69% of cases and metamorphopsia develops in 55% of cases after 2 years of follow-up. Nearly half of patients progress to a macular hole or retinal detachment after 3 years without treatment.
Surgery counteracts this decline. Published results report:
- A gain of more than 2 Snellen lines in 55% of cases.
- Regression of schisis on OCT in 73% of cases.
- Often delayed recovery, which may continue over 6 months to more than one year.
Favorable prognostic factors include: relatively preserved preoperative visual acuity, short duration of symptom progression, and axial length less than 28 mm. Conversely, poor prognostic factors include schisis thickness greater than 500 µm, the presence of vitreomacular traction, foveolar detachment, macular hole, or associated retinal detachment.
FAQ: myopic foveoschisis
What exactly is myopic foveoschisis?
Myopic foveoschisis is a progressive splitting of the retinal layers at the macula, occurring in patients with high myopia. It results from complex tractional forces that stretch and dissociate the neuroretina. The disease is diagnosed by OCT and may remain asymptomatic for a long time before progressing to more severe complications such as a macular hole or retinal detachment.
Does myopic foveoschisis always cause vision loss?
No, many cases of myopic foveoschisis are discovered incidentally during an OCT examination, without any vision loss perceived by the patient. At the pure retinoschisis stage, visual acuity may remain between 20/30 and 20/60. It is primarily when a foveolar detachment or macular hole develops that vision loss becomes significant. Regular monitoring is therefore essential.
How is myopic foveoschisis surgery performed?
The reference procedure is vitrectomy, performed under local or regional anesthesia. The surgeon proceeds with posterior hyaloid detachment, dissection of any epiretinal membranes, and, depending on the case, peeling of the internal limiting membrane. Gas tamponade may be added if a macular hole is present. The procedure typically lasts between 45 minutes and 1 hour 30 minutes, depending on the complexity of the case.
Is myopic foveoschisis surgery painful?
The procedure is performed under local or regional anesthesia, making it painless during the surgical act. Postoperatively, mild discomfort, a foreign body sensation, or tearing may be experienced for a few days. Anti-inflammatory and antibiotic eye drops are prescribed to ensure comfort and prevent complications.
How long does visual recovery take after myopic foveoschisis surgery?
Visual recovery after myopic foveoschisis surgery is often progressive and delayed. It may continue over a period of 6 months to more than one year after the procedure. The best outcomes are observed in patients whose preoperative visual acuity was relatively preserved and whose symptom duration was short. Regular OCT follow-up allows documentation of the progressive reattachment of the retina.
What are the risks of myopic foveoschisis surgery?
As with any vitreoretinal surgery, the procedure carries risks: acceleration of cataract formation (common in phakic patients), development of a secondary macular hole, postoperative retinal detachment, or development of chorioretinal atrophy. These complications remain relatively rare and are weighed against the risk of unfavorable spontaneous progression of untreated myopic foveoschisis.
When can driving and sports be resumed after the surgery?
In the case of gas tamponade, driving is contraindicated until the gas bubble has completely resorbed (generally 2 to 6 weeks depending on the gas used). Air travel is also prohibited during this period. Resumption of gentle physical activities can be considered after 2 to 3 weeks, while intense sports or activities involving impacts should be deferred for at least 4 to 6 weeks. Dr Julien Gozlan tailors these recommendations to each individual situation.
When to consult Dr Julien Gozlan?
If you have high myopia and notice a progressive decrease in your visual acuity, metamorphopsia (distortion of straight lines), increasing difficulty reading, or the appearance of a central scotoma (dark spot in the center of your vision), it is important to promptly consult an ophthalmologist specializing in retinal conditions. An OCT examination will allow screening for possible myopic foveoschisis and assessment of its severity. Likewise, any highly myopic individual, even if asymptomatic, should benefit from regular follow-up including macular OCT in order to detect this condition early and monitor its progression.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan welcomes you at the Paris – Auteuil Ophthalmology Practice for the diagnosis, follow-up, and surgical management of myopic foveoschisis. As a specialist in vitreoretinal surgery, he has a comprehensive technical platform including latest-generation OCT and a dedicated operating suite, to provide you with personalized and reassuring care at every stage.
Book an Appointment on DoctolibFurther reading
- Vitrectomy: procedure and postoperative course: everything you need to know about this reference surgical procedure for vitreoretinal conditions.
- Macular hole: causes, diagnosis, and treatment: understanding this common complication of myopic foveoschisis and its management.
- Macular epiretinal membrane: a condition often associated with high myopia foveoschisis, explained in detail.
- OCT: optical coherence tomography: the key examination for the diagnosis and follow-up of macular and retinal diseases.