
Vitreous hemorrhage refers to the presence of blood in the vitreous, the transparent gel that fills the inside of the eye. It often causes a sudden decrease in vision, the appearance of a dark veil or a "shower of soot". Some forms are uncomplicated and resolve on their own, while others conceal a retinal detachment or severe vascular disease. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, explains the causes, symptoms, diagnostic tests (OCT, ultrasound) and treatments of vitreous hemorrhage.
What is a vitreous hemorrhage?
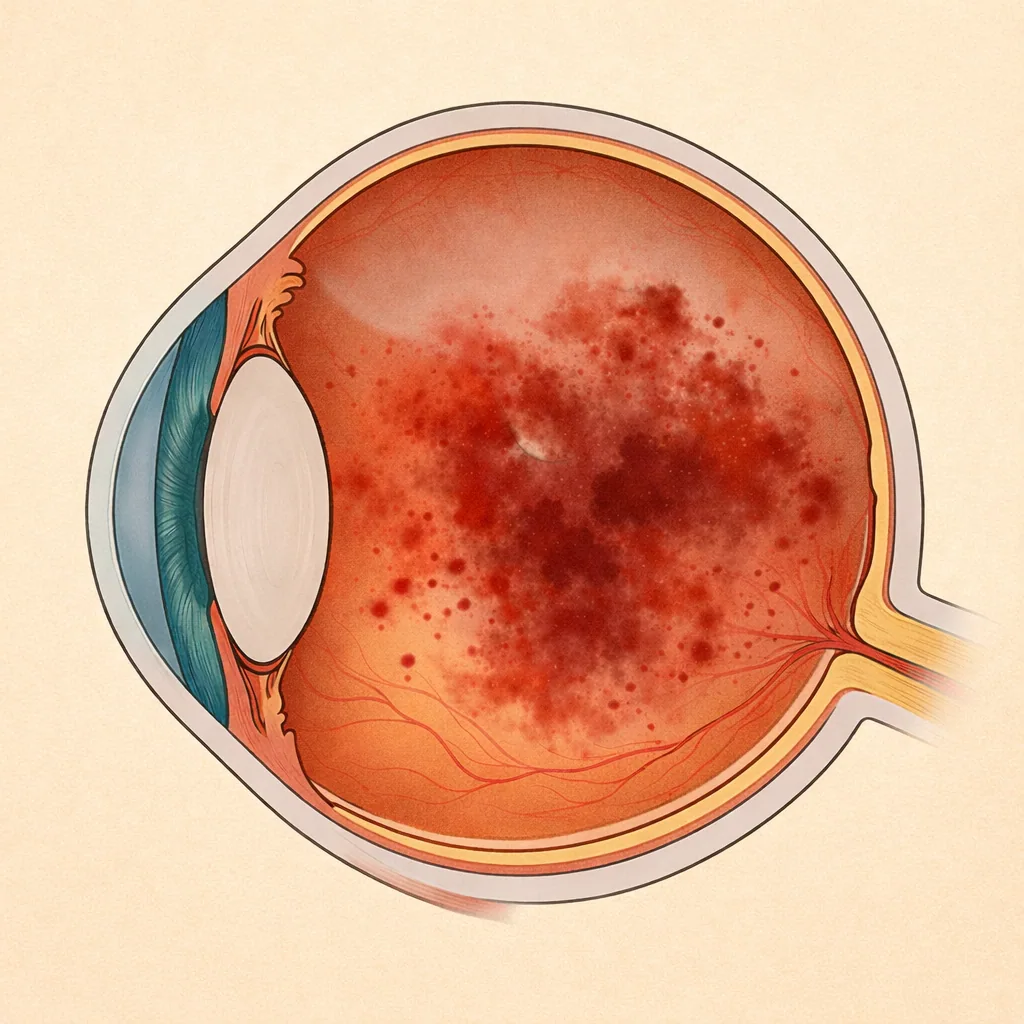
A vitreous hemorrhage occurs when blood diffuses into the vitreous, instead of remaining confined within the retinal or choroidal vessels. The blood mixes with the vitreous gel and forms clumps or sheets that obscure the retina.
Depending on the severity of the bleeding, vitreous hemorrhage can be:
- Moderate: small clumps, "shower of soot", vision still partially preserved;
- Severe: nearly complete red or dark veil, with only light perception remaining;
- Pre-retinal or "sheet-like": a pocket of blood in contact with the retina or beneath the posterior hyaloid.
Vitreous hemorrhage is not a disease in itself, but rather a symptom of an underlying retinal or vascular condition that must be identified.
Symptoms: when should you suspect a vitreous hemorrhage?
Symptoms most often appear suddenly, in one eye:
- Sudden vision loss, sometimes upon waking or during physical exertion;
- Sensation of a red or dark veil in front of the eye;
- "Shower of floaters", numerous mobile black spots or strands;
- Light perception preserved, but details impossible to distinguish;
- Rarely, preceding floaters followed by rapid worsening.
A vitreous hemorrhage should be considered a reason for prompt evaluation, especially if you already have a retinal condition (diabetes, AMD, high myopia, etc.) or if the vision loss is very significant.
Main causes and risk factors
Among the major causes of vitreous hemorrhage are:
- Proliferative diabetic retinopathy: growth of fragile neovessels that bleed easily;
- Retinal vein occlusions (for example, a central retinal vein occlusion) with secondary neovascularization;
- Retinal tear or retinal detachment: a retinal break may be accompanied by bleeding into the vitreous, heralding a retinal detachment;
- Ocular trauma (direct blow, ball, sports accident);
- Choroidal neovascularization (high myopia, certain maculopathies);
- Postoperative complication (after retinal surgery or cataract surgery);
- Coagulation disorders or anticoagulant/antiplatelet therapy in the context of fragile vasculature.
The most common risk factors are poorly controlled diabetes, high blood pressure, advanced age, high myopia and certain types of trauma. Identifying the cause determines the treatment and visual prognosis.
Diagnosis: fundus examination, OCT and ultrasound
The workup begins with a comprehensive examination by an ophthalmologist:
- Measurement of visual acuity and comparison with baseline values;
- Slit-lamp examination to look for traces of blood in the anterior chamber or on the lens;
- Fundus examination after dilation: possible only if the hemorrhage is not too dense.
When blood obscures the retina, fundus details can no longer be seen. The examination is then supplemented with imaging:
- Macular OCT, if transparency allows, to assess the condition of the macula and look for edema (macular OCT);
- B-scan ocular ultrasound: a key examination when the retina is no longer visible, to detect a retinal detachment, a tear or a tumor;
- Possibly, fluorescein angiography once the hemorrhage clears, to analyze neovessels and areas of ischemia (fluorescein angiography).
Imaging: what is assessed on OCT and ultrasound
In practice, imaging helps guide management. The main features analyzed are:
On ocular ultrasound
- Appearance of mobile hyperechoic clumps in the vitreous (recent hemorrhage);
- Presence or absence of a retinal detachment (thickened membrane, "tent-shaped", attached to the optic nerve);
- Localized membrane that may correspond to a retinal tear or a vascular scar;
- Exclusion of an intraocular mass (tumor, melanoma).
On macular OCT
- Detection of macular edema (diabetic, venous, inflammatory);
- Assessment of macular structure (epiretinal membrane, macular hole, vitreomacular traction);
- Status of the outer retinal layers (ellipsoid zone, external limiting membrane) to estimate visual potential after treatment.
These findings are used to stratify risk: uncomplicated vitreous hemorrhage that can be monitored, versus hemorrhage masking a serious retinal condition requiring prompt surgery.
Treatment of vitreous hemorrhage
Treatment depends on the severity of the hemorrhage, its cause and the condition of the underlying retina.
1) Observation and treatment of the underlying cause
A moderate vitreous hemorrhage, without retinal detachment or serious lesion, can sometimes be monitored. The blood gradually resorbs over several weeks or months. At the same time, the underlying cause is treated:
- Optimizing diabetes control and cardiovascular risk factors;
- Laser photocoagulation of ischemic neovessels once the retina becomes visible again;
- Possible adjustment of certain anticoagulant therapies (in coordination with the primary care physician or cardiologist).
2) Intravitreal injections
When vitreous hemorrhage is related to neovascularization (diabetic retinopathy, vein occlusion, certain forms of AMD), intravitreal anti-VEGF injections or corticosteroids may be offered, once visibility permits the procedure (intravitreal injections).
3) Vitrectomy for vitreous hemorrhage
In cases of severe and persistent hemorrhage, suspected retinal detachment or major visual impairment, the standard treatment is vitrectomy:
- Micro-incisions in the white of the eye;
- Aspiration of the blood-laden vitreous;
- Simultaneous treatment of retinal lesions (endolaser, membrane peeling, gas tamponade, etc.).
This procedure allows clearing of the visual axis and direct treatment of the cause. It is described in detail on the dedicated vitrectomy page.
Visual prognosis and follow-up
The prognosis of a vitreous hemorrhage depends primarily on:
- The condition of the retina (presence or absence of detachment, macular ischemia, pre-existing damage);
- The speed of management in cases of retinal tear or retinal detachment;
- The underlying cause (advanced diabetes, severe vein occlusion, significant trauma, etc.).
In many cases, vision improves significantly after hemorrhage resorption or after vitrectomy. However, if the macula was already affected, recovery may remain partial. Regular follow-up with fundus examinations, OCT and sometimes ultrasound is essential.
Practical advice for patients
- Seek prompt evaluation in case of a sudden dark veil, a shower of numerous black spots or significant vision loss in one eye.
- Avoid driving as long as vision is unstable or severely reduced.
- If you have diabetes, maintain strict blood sugar control and regular retinal monitoring.
- Inform your ophthalmologist of any anticoagulant or antiplatelet therapy.
- Keep all follow-up appointments even if vision seems to be improving.
- After vitrectomy, strictly follow postoperative instructions (head positioning, eye drops, any activity restrictions).
Frequently asked questions about vitreous hemorrhage
Is it an emergency?
Yes, a vitreous hemorrhage warrants prompt evaluation, especially if the vision loss is sudden or significant. The goal is to identify the cause (neovascularization, retinal tear, retinal detachment, trauma, vein occlusion, etc.) and to verify that there is no complication requiring urgent treatment, particularly a retinal detachment or a retinal tear.
Is a vitreous hemorrhage painful?
Generally, no: there is no pain. The discomfort is primarily visual (veil, blurriness, spots, vision loss, mobile "cloud"). Pain, significant redness or light sensitivity point more toward an associated condition (trauma, inflammation, elevated intraocular pressure) and should be reported.
Will the blood resolve on its own?
Sometimes yes, especially if the hemorrhage is mild and the cause is controlled. Resorption can take several weeks, sometimes several months, as the vitreous clears slowly. If the hemorrhage is dense, if it persists, if it recurs, or if it prevents adequate examination of the retina, a vitrectomy may be recommended to evacuate the blood and treat the cause (laser, neovascularization management, etc.).
Can it lead to permanent vision impairment?
The risk of lasting damage depends mainly on the underlying disease and how quickly it is managed (proliferative diabetic retinopathy, vein occlusion, retinal tear or retinal detachment, trauma, etc.). The vitreous hemorrhage itself is often reversible, but it may reveal a serious retinal condition that can threaten vision if left untreated.
Are anticoagulants or antiplatelet agents responsible?
Anticoagulants and antiplatelet agents can promote or worsen bleeding, but they are generally not the sole cause: there is most often an underlying lesion (fragile neovessels, traction, rupture of a small vessel, etc.). You should never modify or stop these medications without the advice of your cardiologist or primary care physician: the decision is made on a case-by-case basis, weighing the benefit-risk ratio.
Can vitreous hemorrhage be prevented?
Prevention mainly involves addressing risk factors and the diseases that weaken retinal blood vessels: good diabetes control, managed blood pressure, regular fundus examinations, screening for and treatment of neovascularization (laser, injections if necessary), and eye protection during sports or activities with a risk of trauma. These measures reduce the risk of bleeding but do not eliminate it entirely.
Can you travel or fly with a vitreous hemorrhage?
An uncomplicated vitreous hemorrhage does not in itself prevent travel. However, if surgery has been performed with gas tamponade, air travel and high altitude are strictly contraindicated as long as the gas is present, because the bubble can expand and dangerously increase pressure inside the eye. Specific instructions are provided on a case-by-case basis depending on the treatment and retinal status.
How much time off work should be expected?
This depends on the density of the hemorrhage, the cause, visual recovery and your occupation (screen work, driving, precision work, heavy lifting). In cases of simple observation, time off is not always necessary but may be required if vision is too impaired. After vitrectomy, a few days to a few weeks off is often recommended, adjusted according to occupational demands (professional driving, working at heights, physical exertion, etc.).
When to consult Julien Gozlan, M.D.?
You should seek prompt evaluation in case of a dark veil, a sudden shower of black spots or vision loss that may suggest a vitreous hemorrhage. A comprehensive examination, including ocular ultrasound and OCT when possible, can confirm the diagnosis, identify the cause and recommend appropriate treatment (observation, laser, injections, vitrectomy).
Julien Gozlan, M.D., ophthalmologist in Paris 16, welcomes you to the practice for a comprehensive retinal evaluation and personalized management of your vitreous hemorrhage and associated conditions.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. performs a comprehensive retinal evaluation (fundus examination, ultrasound, OCT) and discusses the various treatment options with you in cases of vitreous hemorrhage.
Book an AppointmentFurther reading
- Floaters and "eye floaters": when a simple visual disturbance conceals a retinal condition.
- Diabetic retinopathy: screening and management of proliferative forms.
- Age-related macular degeneration (AMD): neovascularization and bleeding risks.
- OCT angiography: detailed analysis of retinal microcirculation without injection.