
OCT angiography (or OCT-A) is a recent imaging technique that allows visualization of blood circulation in the retina and choroid without dye injection. It complements conventional macular OCT and fluorescein angiography. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, explains the principle, indications, and limitations of OCT angiography.
What is OCT angiography?
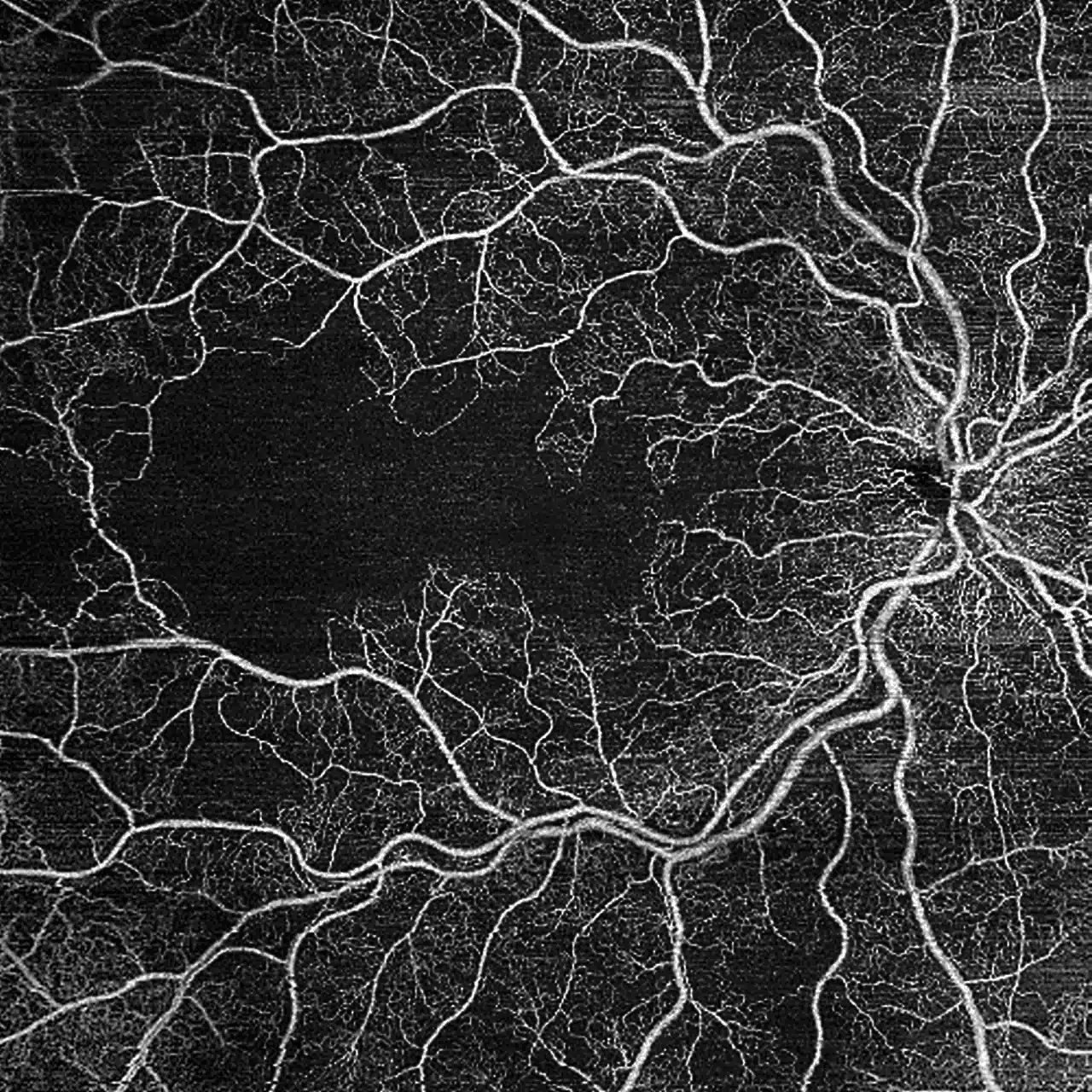
OCT angiography is an advancement of structural OCT. The device acquires very thin cross-sections of the retina, as well as repeated acquisitions at the same location. By analyzing micro-variations in signal between two captures, it detects the movement of red blood cells in small vessels.
From this information, software reconstructs layer-by-layer vascular maps: superficial plexus, deep plexus, choriocapillaris, and more. This produces a true "angiography" without needles or dye injection, based solely on blood movement.
OCT-A: which vascular layers can be analyzed?
One of the major advantages of OCT angiography is segmentation: the image is divided into successive planes to visualize different vascular networks. In practice, the main layers studied are:
- the superficial capillary plexus (close to the retinal surface);
- the deep capillary plexus (often involved in certain macular ischemic conditions);
- the foveal avascular zone (FAZ) and its contours;
- the choriocapillaris;
- sometimes neovascular networks (AMD, high myopia, inflammatory causes).
This "layer-by-layer" analysis helps explain why a patient may experience decreased vision even when structural OCT appears relatively normal: the microcirculation can be affected before visible anatomical changes occur.
In which cases is OCT angiography useful?
OCT angiography is particularly valuable for:
- detecting or monitoring choroidal neovascularization in exudative AMD;
- analyzing macular ischemic areas and the foveal capillary network in diabetic retinopathy;
- studying retinal vein occlusions (central or branch) at the macular level;
- investigating certain uveitic conditions or atypical maculopathies;
- monitoring the effect of intravitreal injections on macular vascularization.
It is particularly valuable when frequent follow-up examinations are needed over time, without having to repeat dye injections each time.
How is an OCT angiography examination performed?
The examination is quick and painless. It is performed in a seated position, with the chin resting on a support and the forehead against a bar. There is no needle and no injection.
You are asked to fixate on a light point inside the device. Within a few seconds, the OCT acquires both structural and "angiographic" images. It is important to remain still and fixate properly, as eye movements can generate image artifacts.
OCT angiography can be performed with or without pupil dilation, depending on the clarity of the ocular media and the expected image quality. Results are available immediately for interpretation.
What OCT angiography shows
OCT angiography provides several types of images:
- conventional OCT cross-sections showing retinal thickness and structure;
- perfusion maps of the macula (superficial plexus, deep plexus);
- visualization of choroidal neovascularization or abnormal networks;
- ischemic areas or capillary rarefaction zones;
- the appearance of the choriocapillaris in certain maculopathies.
The examination thus allows precise localization of vascular abnormalities, assessment of whether they are still active, and monitoring of their progression under treatment.
Interpretation: how is a neovascular membrane identified on OCT-A?
In practice, OCT angiography is very useful for identifying abnormal vascular networks. A choroidal neovascular membrane often appears as a "lace-like" or "bush-like" structure, of varying density, within the deeper layers.
Key features to look for include:
- the presence of a network in a layer consistent with neovascularization;
- its extent (size, borders);
- its organization (fine network versus a "mature" and dense one);
- and most importantly, the correlation with findings on structural OCT (intraretinal/subretinal fluid, irregularities, etc.).
In other words: OCT-A shows the network, while structural OCT often shows the consequences on the retina.
OCT angiography, conventional OCT, and fluorescein angiography: what are the differences?
Structural macular OCT primarily shows the architecture of retinal layers, OCT angiography focuses on microcirculation, and fluorescein angiography visualizes dye diffusion through the vessels.
In practice:
- OCT angiography is non-invasive and can be repeated as often as necessary;
- it provides excellent visualization of macular neovascularization, even when minimally exudative;
- however, it does not directly show dye leakage or certain far-peripheral vessels.
In many cases, OCT-A and fluorescein angiography are complementary: the former provides a detailed vascular map, while the latter shows the intensity of leakage and broader retinal perfusion.
Limitations and artifacts of OCT angiography
Like any examination, OCT angiography has its limitations. Images can be difficult to interpret in cases of:
- poor fixation (excessive eye movement);
- opaque media (dense cataract, significant vitreous opacities);
- large hemorrhages obscuring the macula.
The device can also generate artifacts (double contours, vascular "projection," false flow voids) that require specific expertise to recognize. The value of OCT-A is always assessed in conjunction with the clinical examination and other available imaging.
What are the practical benefits for the patient?
For the patient, OCT angiography provides:
- improved detection of certain macular neovascular membranes;
- detailed monitoring of macular microcirculation during treatment;
- a reduction in the number of dye injections, particularly in chronic conditions;
- a better understanding of the relationship between imaging findings and perceived vision.
In practice, OCT-A helps adjust the frequency of intravitreal injections, confirm macular stability, or detect disease reactivation earlier.
Frequently asked questions about OCT angiography
Is it painful?
No, the examination is completely painless. There is no needle, no injection, and no contact with the eye in the vast majority of cases. You simply fixate on a target for a few seconds while the device records the images.
Do I need to fast beforehand?
No, no dietary preparation is required. You can eat and drink normally before an OCT angiography.
Can I drive after an OCT angiography?
If the pupils have been dilated, vision may be blurry and sensitive to glare for a few hours: it is then advisable to avoid driving right after the examination. Without dilation, driving is generally possible, provided your vision is comfortable and stable.
Does OCT angiography replace fluorescein angiography?
No, not entirely. OCT angiography visualizes vessels by mapping blood flow, but it does not directly show leakage as fluorescein angiography does. It also provides less coverage of the retinal periphery. In many situations, both examinations are complementary, and the choice depends on the clinical question (neovascular activity, edema, ischemia, etc.).
Why are artifacts mentioned in the images?
Because OCT-A reconstructs vascularization from micro-variations in signal between multiple acquisitions. Certain elements can then "distort" the image: eye movements, blinking, cataract, opacities, shadow projections, or segmentation errors. These artifacts can create false vessels, mask real flow, or give the impression of an abnormality. This is why interpretation is always performed by cross-referencing structural OCT, B-scan, and segmentation quality.
In which cases is OCT-A most useful in practice?
It is particularly useful for detecting neovascularization (AMD, high myopia, pachychoroid spectrum disorders), monitoring certain vascular conditions (diabetic retinopathy, vein occlusions), analyzing macular microcirculation, and comparing changes over successive follow-up visits, without injection. It also helps detect neovascular networks that are poorly visible on conventional angiography in certain contexts.
How long does the examination take?
The examination takes a few minutes. The acquisition itself takes only a few seconds per eye, but it may sometimes be necessary to repeat a capture if fixation was not optimal, or to acquire multiple scan fields (3×3, 6×6, 12×12) depending on the indication.
Does OCT-A need to be repeated frequently?
That depends on the condition and its activity. When monitoring neovascularization or treatment with intravitreal injections, OCT-A may be repeated to monitor microcirculation, look for reactivation, and complement structural OCT. In more stable situations, it is performed only as needed, when the examination provides useful information for therapeutic decision-making.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. uses OCT angiography alongside the clinical examination to analyze your macula in detail, adjust treatment frequency, and ensure personalized monitoring of retinal diseases.
Book an AppointmentFurther reading
- Central retinal vein occlusion (CRVO): assessment and treatment of macular edema.
- Branch retinal vein occlusion (BRVO): symptoms, OCT, and injections.
- Intravitreal injections: procedure, efficacy, and follow-up.
- Fluorescein angiography: imaging with dye injection.