
Branch retinal vein occlusion (BRVO) is a blood circulation disorder affecting a branch of the retinal vein. It can cause vision loss, sometimes sudden, and requires close ophthalmological follow-up. Dr Julien Gozlan, ophthalmic surgeon, explains the causes, symptoms, examinations, and treatments to be implemented.
What is branch retinal vein occlusion (BRVO)?
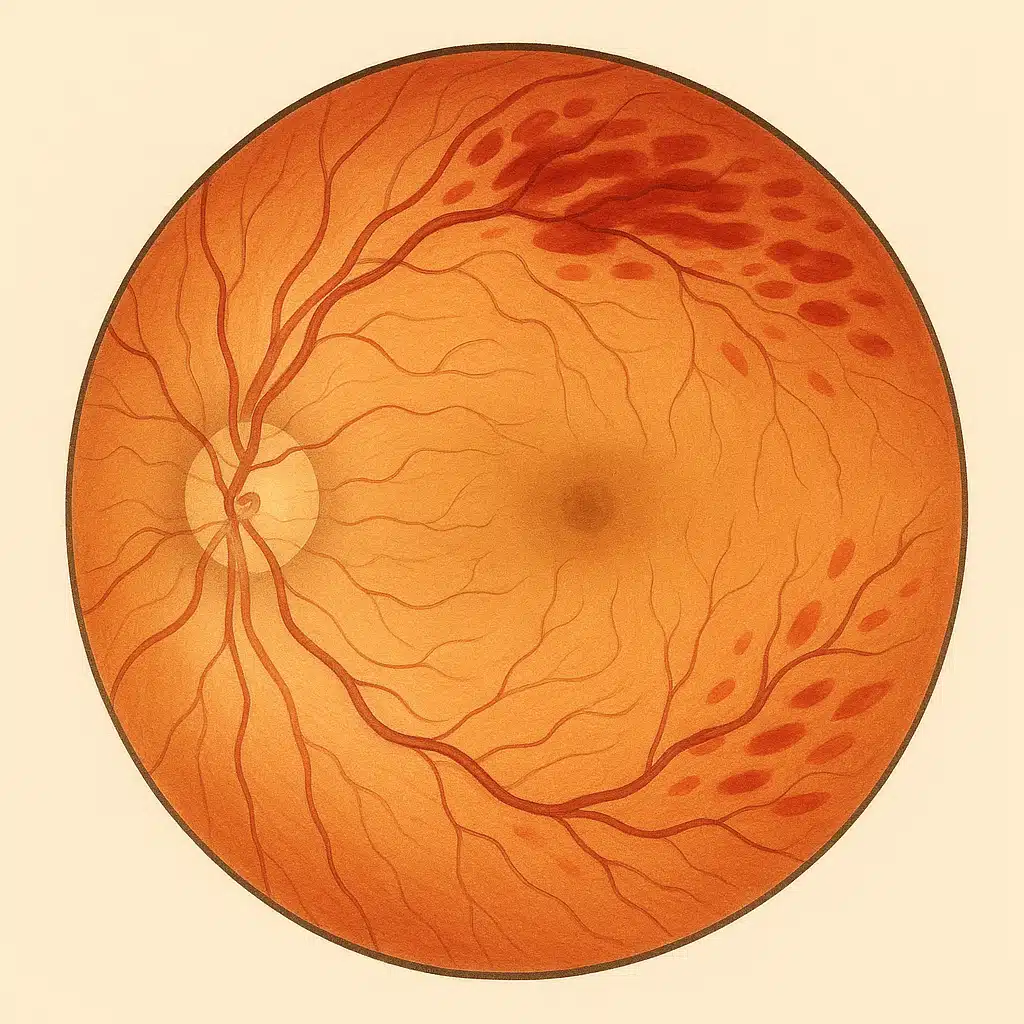
A branch retinal vein occlusion occurs when a blockage develops in a branch vein of the retina. Blood stagnates, the veins dilate and become tortuous, hemorrhages may appear in the affected area, and the retina may swell (macular edema). Unlike CRVO (central retinal vein occlusion), branch retinal vein occlusion affects only one sector of the retina.
What are the risk factors?
This condition more commonly affects people over 50 years of age. The most frequent risk factors are: high blood pressure, glaucoma and ocular hypertension, diabetes, smoking, dyslipidemia (cholesterol), and coagulation disorders. Cardiovascular monitoring and management of risk factors reduce the risk of recurrence.
Symptoms of BRVO
Signs vary depending on the location of the branch retinal vein occlusion (BRVO): vision loss (often upon waking), a gray or dark spot in the visual field, distortion of lines, or blurred vision. If the macula is affected, the visual impairment is more pronounced, particularly for reading or fine details.
Essential examinations
Diagnosis is based on fundus examination. Two imaging tests are commonly performed:
- OCT (Optical Coherence Tomography): detects and analyzes macular edema and monitors its progression.
- Fluorescein angiography: confirms the diagnosis and detects complications (ischemic areas or retinal neovascularization).
These examinations allow the treatment of branch retinal vein occlusion to be tailored and follow-up to be planned as closely as possible to the progression of the macula.
Treatment of branch retinal vein occlusion
The goal is to reduce macular edema, prevent complications, and optimize visual recovery. Several options may be offered:
- Intravitreal injections of anti-VEGF agents or corticosteroids: the standard treatment to reduce edema and improve vision.
- Retinal laser: photocoagulation of poorly perfused retinal areas to prevent the risk of neovascularization or hemorrhage. A macular grid laser may be considered in certain situations.
- Management of risk factors: high blood pressure, ocular hypertension or glaucoma, cardiovascular assessment, blood sugar and lipid control, smoking cessation.
In most cases, treatment of branch retinal vein occlusion extends over several months, with an initial injection regimen followed by a schedule adapted according to macular OCT.
Visual prognosis
The outcome depends on the initial severity, macular involvement, and how quickly treatment is initiated. Many patients recover useful vision when macular edema resolves with treatment. The earlier branch retinal vein occlusion is managed, the better the functional prognosis, particularly with appropriate follow-up by macular OCT, and with suitable treatment such as intravitreal injections.
FAQ: frequently asked questions about branch retinal vein occlusion (BRVO)
Is a BRVO always an ophthalmological emergency?
Yes, a branch retinal vein occlusion should be managed promptly, even if the vision loss seems moderate. It is not a life-threatening emergency, but it is advisable to consult within the days following the onset of symptoms (blurred vision, gray spot, line distortion). An early assessment allows the diagnosis to be confirmed, any macular edema to be evaluated, and treatment to be initiated at the most beneficial time for your vision.
Does vision return to normal after a BRVO?
The outcome varies from one patient to another. When macular edema responds well to treatment (intravitreal injections, possible laser), many patients recover satisfactory functional vision for daily life. However, a slight decrease in visual acuity or difficulty with fine reading may persist. The prognosis depends on how quickly treatment is initiated, the location of the affected area, and the presence of other eye conditions (glaucoma, diabetic retinopathy, etc.).
What is the difference between BRVO and CRVO for the patient?
In a BRVO, only a branch vein of the retina is affected, which limits the involvement to one sector of the visual field. In a CRVO, it is the main vein that becomes blocked, and the involvement is more widespread. In practical terms, a BRVO may cause a sometimes localized impairment (blurred area, gray spot), whereas a CRVO often results in more global and more severe vision loss. Management remains rigorous in both cases (macular OCT, angiography, injections, risk factor control) to protect the macula and limit visual sequelae.
How long does treatment for a BRVO last?
Treatment most often extends over a prolonged period. An initial phase generally includes several closely spaced intravitreal injections (for example monthly), then the frequency is adjusted based on macular OCT findings and edema stability. In some patients, the treatment plan may extend over several months to more than a year, with visits spaced further apart once the retina remains dry. Do not be discouraged: these repeated treatments aim to give the eye the best chance of recovering and maintaining stable long-term vision.
Is there a risk for the other eye or of having another BRVO later?
Yes, a risk of recurrence exists, either in the same eye or in the other eye, especially if cardiovascular risk factors are not addressed (high blood pressure, diabetes, high cholesterol, coagulation disorders, smoking). This is why a BRVO should always lead to a comprehensive general assessment alongside ophthalmological management. Good blood pressure control, better diabetes management, and smoking cessation significantly reduce the risk of a new retinal vascular event.
Will I be able to continue working and driving after a BRVO?
This depends on the final vision of the affected eye and any impact on binocular vision. Many patients can return to work and driving once vision has sufficiently recovered, particularly if the other eye remains healthy. However, certain visually demanding occupations (precision work, professional driving) may require a longer period off work or workplace adjustments. Legal driving criteria are assessed on a case-by-case basis with your ophthalmologist, who can provide personalized advice.
What can I do myself to protect my retina after a BRVO?
Beyond ocular treatments, your role is essential. It involves optimally controlling all risk factors: regularly taking prescribed medications for blood pressure and cholesterol, monitoring your diabetes with your physician, quitting smoking, engaging in appropriate physical activity, and maintaining a balanced diet. Regarding your vision, follow the schedule for OCT examinations and injections, and seek earlier consultation if you experience new vision loss or distortion. These combined measures increase your chances of maintaining useful vision over the long term after a branch retinal vein occlusion.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan sees patients for the diagnosis, follow-up by macular OCT, and treatment of branch retinal vein occlusion (BRVO) (intravitreal injections, laser, risk factor management).
Book an AppointmentFurther reading
- Macular OCT: the reference examination for monitoring macular edema.
- Intravitreal injections: the key treatment for branch retinal vein occlusion.
- Central retinal vein occlusion (CRVO): another form of retinal vein occlusion.
- Diabetic macular edema: understanding other causes of macular edema.
- AMD: when the macula is affected by an age-related disease.
- Branch retinal vein occlusion: urgent consultation : rapid management to limit visual sequelae.