
Retinal laser (or retinal photocoagulation) is a major treatment in ophthalmology used to protect the retina and prevent certain serious complications, such as retinal detachment or vision loss related to diabetes or retinal vein occlusions. It does not "fix" everything, but it often helps to stabilize the situation and limit the risk of worsening. Julien Gozlan, M.D., ophthalmologist in Paris 16, explains the indications for this treatment, the practical course of sessions, the expected outcomes, and the precautions to be aware of.
What is retinal laser treatment?
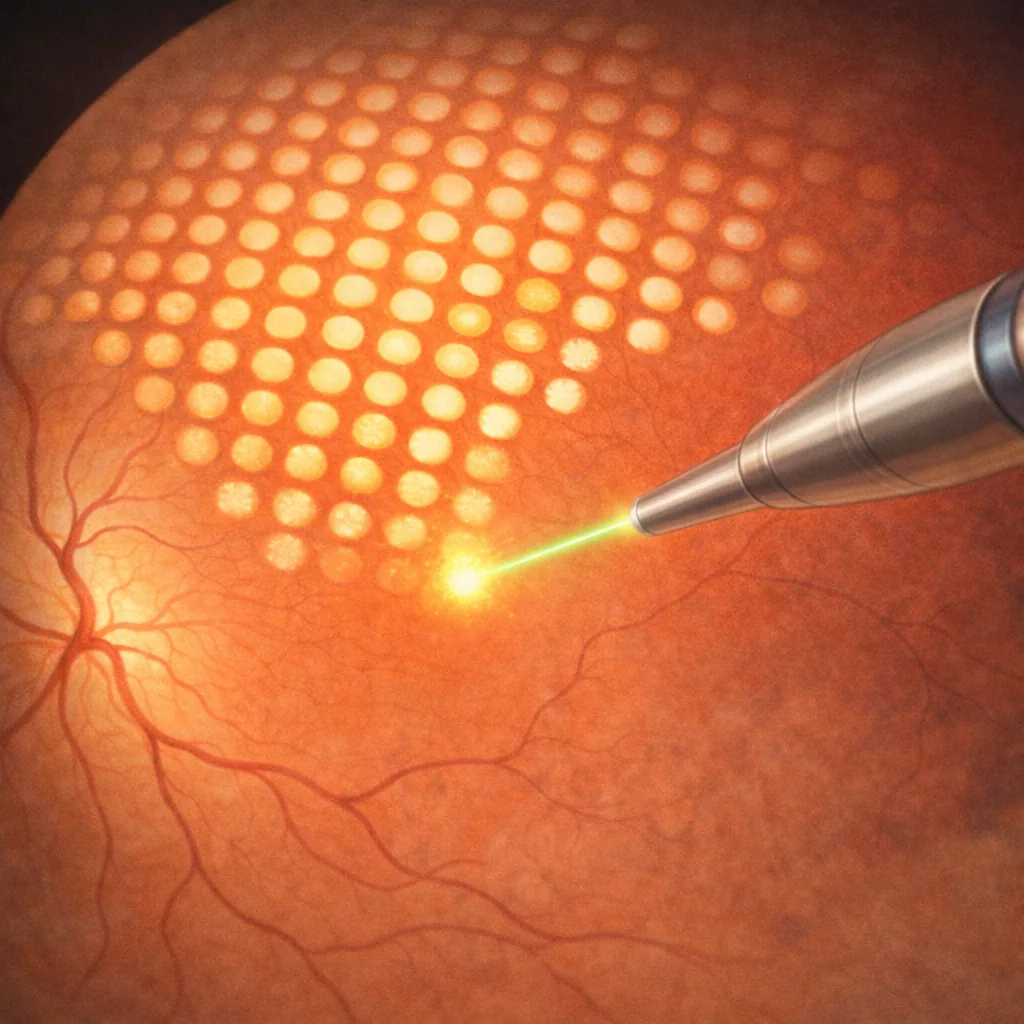
Retinal laser treatment involves applying highly focused light impacts to specific areas of the retina. The light energy is converted into heat, creating small scar adhesions or modifying the metabolism of retinal tissues.
The goal is not to "improve" vision like a pair of glasses, but to stabilize the retina:
- by reinforcing certain fragile areas (tears, degenerations);
- by reducing ischemia (lack of oxygen) in severe retinopathies, such as diabetic retinopathy;
- by treating macular edema in certain well-defined indications.
There are different laser treatment patterns (focal, grid, panretinal), tailored to each condition and each lesion topography.
Main indications for retinal photocoagulation
The most common situations in which retinal laser treatment may be recommended are:
- Proliferative or severe diabetic retinopathy: panretinal photocoagulation reduces ischemia and causes abnormal neovessels to regress.
- Diabetic macular edema or edema following central retinal vein occlusion (CRVO) or branch retinal vein occlusion (BRVO), in selected cases.
- Retinal tears or early retinal detachment: laser barrage around the lesion to prevent extension.
- At-risk peripheral degenerations (lattice degeneration, snail-track degeneration, etc.) in highly myopic patients or those with a history of retinal detachment.
- Certain forms of ischemic retinopathies (extensive vein occlusions, peripheral ischemia) to reduce the risk of neovascularization.
The choice of treatment is always made on a case-by-case basis, after a thorough retinal examination and analysis of imaging studies (fundus examination, macular OCT, angiography, etc.).
How does a retinal laser session proceed?
Most sessions are performed on an outpatient basis, in the office or clinic, without hospitalization. In practice:
- dilating eye drops are instilled to widen the pupil;
- a topical anesthetic in drop form is applied to numb the surface of the eye;
- a special contact lens is sometimes placed on the eye, with gel, to better focus the light beam on the retina.
The patient sits at a slit lamp, as for a standard examination, but the ophthalmologist uses a treatment attachment coupled to the lamp. The duration generally ranges from 10 to 30 minutes depending on the type of treatment and the number of impacts.
During the session, you may perceive flashes of light and, occasionally, a slight tingling or warm sensation. Most patients describe the procedure as impressive but tolerable, with transient discomfort rather than actual pain.
Retinal laser treatments: the main types
Panretinal photocoagulation (diabetic retinopathy, ischemia)
Panretinal photocoagulation involves applying numerous light impacts to the peripheral retina, while sparing the macula. It is primarily used in severe forms of diabetic retinopathy or certain ischemic vein occlusions.
This treatment helps to reduce ischemia and thus cause neovessels to regress, decreasing the risk of vitreous hemorrhage or neovascular glaucoma. It may sometimes be performed over several sessions, spaced a few days or weeks apart.
Focal or grid laser photocoagulation (macular edema)
In certain cases of macular edema (diabetic or secondary to vein occlusion), photocoagulation treatment may be recommended:
- focal treatment targets precise leakage points near the macula;
- grid photocoagulation applies multiple impacts across a more diffuse edematous area.
Today, this strategy is often combined with, or sometimes replaced by, intravitreal injections, particularly anti-VEGF agents. The choice depends on the location of the edema, its severity, and current guidelines.
Laser barrage for retinal tears
In the presence of a retinal tear, photocoagulation is used to create a retinal barrage: a ring of impacts around the lesion. This creates an area of adherent scar tissue that "seals" the retina to the eye wall, reducing the risk of fluid seeping underneath and causing a retinal detachment.
The treatment can be completed in one or more sessions depending on visibility, patient tolerance, and the retina's response.
Recovery, effectiveness, and limitations of retinal laser
After retinal photocoagulation, vision may be temporarily blurred, mainly due to dilation, glare, and sometimes mild retinal edema. Headaches or a sensation of eye fatigue are possible.
The expected outcomes are:
- in proliferative retinopathy: regression of neovessels and reduced risk of hemorrhage or neovascular glaucoma;
- in retinal tears: stabilization of the retina and prevention of detachment;
- in macular edema (specific indications): reduction of edema or complement to injection therapy.
However, this technique has limitations:
- it does not always allow recovery of vision that has already been severely impaired;
- additional treatments (further sessions, intravitreal injections, surgery) may be necessary;
- depending on the indication, it may cause a reduction in peripheral visual field or scotomas noticeable in low-light conditions.
Risks and possible side effects
This procedure is well-established and widely used, but like any medical procedure, it carries risks that are rare but possible:
- temporary visual discomfort, glare, blurred vision for a few hours;
- small localized retinal or vitreous hemorrhages;
- reduction of peripheral visual field after extensive panretinal treatment;
- rare macular damage if an impact lands too close to the fovea;
- very rarely, transient worsening of macular edema.
Detailed information is provided before the procedure, with an assessment of the benefit-risk ratio based on your individual situation.
Practical advice before and after retinal laser treatment
Some useful recommendations for patients scheduled for retinal photocoagulation:
- preferably come accompanied, as vision may be blurred after dilation;
- inform the ophthalmologist of any systemic medications (anticoagulants, antidiabetic drugs, etc.) and your medical history;
- after the session, avoid driving immediately, especially at night;
- follow the prescribed eye drops after treatment (anti-inflammatory drops, artificial tears, etc.);
- seek emergency consultation if you experience a sudden drop in vision, the appearance of a dark curtain, intense flashes, or significant pain.
FAQ: laser and the retina
Is retinal laser treatment painful?
Most patients describe it as a tolerable procedure. The eye is numbed with drops, which prevents outright pain. You may feel tingling, warmth, or eye fatigue, and occasionally some slightly more sensitive impacts, but the session is generally well tolerated. If significant discomfort occurs, do not hesitate to report it during the treatment so that the pace or delivery of impacts can be adjusted.
How many sessions are needed?
It depends entirely on the retinal condition. A tear barrage can sometimes be completed in a single session, while panretinal photocoagulation for severe diabetic retinopathy often requires several sessions spaced a few days or weeks apart. The ophthalmologist outlines the planned treatment schedule from the start, which may be adjusted based on how the condition evolves.
Can you drive after a session?
Immediately after the session, vision is often blurred due to dilation and glare. It is therefore recommended not to drive immediately, particularly at night or for long trips. As a general rule, functional vision returns within a few hours. You may resume driving when you feel visually comfortable and safe, following the advice given at the practice.
Does the laser replace intravitreal injections?
No, these are complementary treatments. In many conditions (diabetes, vein occlusions, AMD), intravitreal injections are the standard treatment for macular edema, while photocoagulation primarily addresses ischemic areas or retinal tears. Depending on the case, one, the other, or a combination of both may be recommended to optimize the visual outcome and stabilize the retina.
Can laser treatment cause vision loss?
In some cases, there may be a reduction of peripheral visual field or decreased vision in very dim lighting. However, this treatment is recommended when the natural risk of the disease (hemorrhage, detachment, neovascular glaucoma) is more serious than this peripheral impact. The goal remains to preserve central vision and avoid far more severe complications for eyesight.
What is the difference between retinal laser and YAG laser?
Retinal laser targets the retina to treat tears, retinopathies, or edema by creating small controlled burns. The YAG laser is primarily used for capsulotomy after cataract surgery (posterior capsule opacification) or for certain iridotomies in angle-closure glaucoma. It does not act on the retina but on other structures of the eye. These are therefore two very different technologies with two very different indications.
Are there specific precautions with anticoagulants or diabetes?
Treatment with anticoagulants or antiplatelet agents is not a contraindication. They may promote small superficial hemorrhages, but these are usually not serious. However, poorly controlled diabetes increases the risk of retinopathy and warrants closer monitoring. Before extensive photocoagulation (panretinal, for example), it is preferable to optimize glycemic control as much as possible in coordination with the primary care physician or diabetologist.
When should you consult Julien Gozlan, M.D.?
You may seek an opinion if you have been told about diabetic retinopathy, retinal vein occlusion, retinal tear, or if retinal laser treatment has been recommended and you would like a second opinion or detailed explanations about the benefits of the treatment.
Julien Gozlan, M.D., ophthalmologist in Paris 16, performs a comprehensive fundus examination and appropriate imaging studies (OCT, angiography, ultrasound if needed), then discusses the various treatment options with you, based on your visual and overall health status.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. welcomes you at the Paris – Auteuil Ophthalmology Practice to assess the condition of your retina, confirm or rule out the indication for treatment, and develop a personalized follow-up plan with you.
Book an AppointmentFurther reading
- Diabetic retinopathy: stages, symptoms, and treatments.
- Retinal detachment: warning signs and surgical management.
- Macular OCT: the reference imaging technique for retinal analysis.
- Intravitreal injections: the role of anti-VEGF agents and corticosteroids in retinal diseases.