
Irvine-Gass syndrome refers to cystoid macular edema occurring after cataract surgery. It presents as blurred or distorted central vision several weeks after an apparently uneventful procedure. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, explains the symptoms, the role of OCT, and the treatments for Irvine-Gass syndrome.
What is Irvine-Gass syndrome?
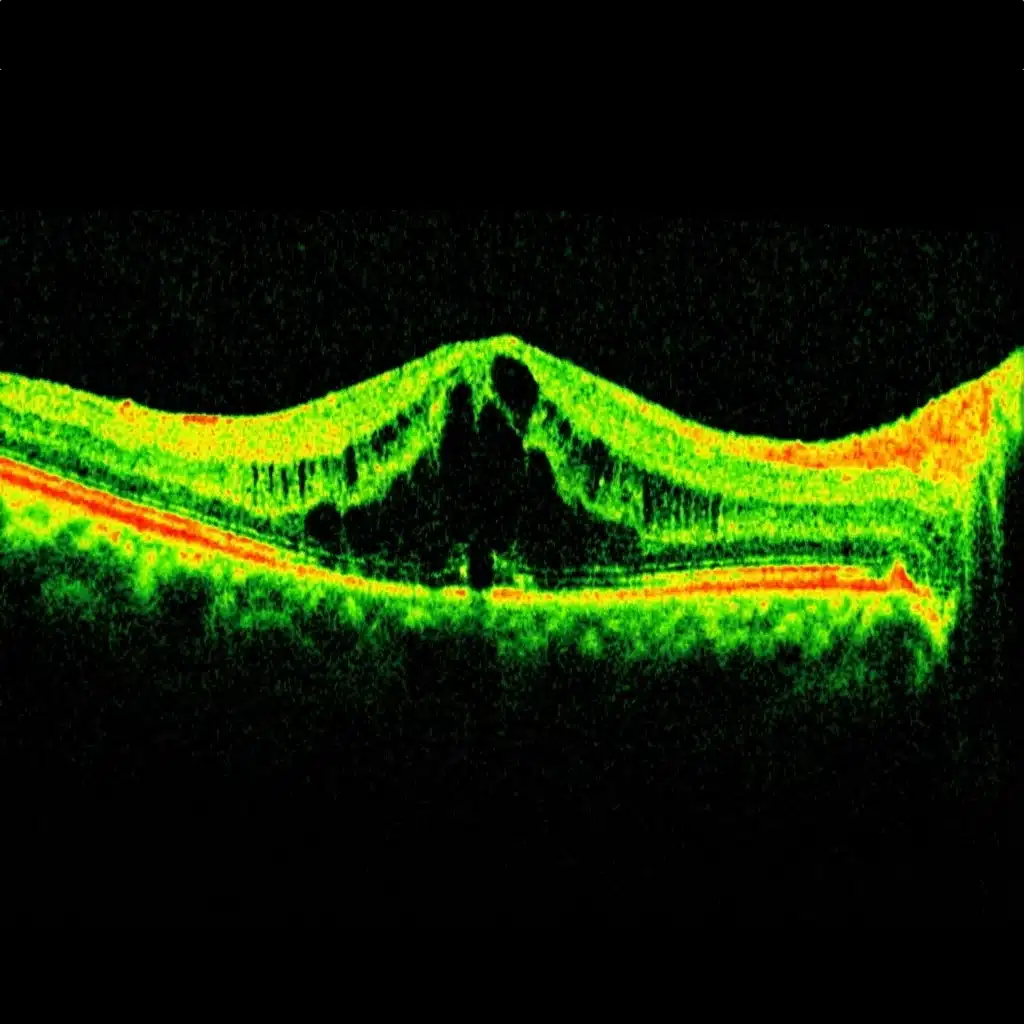
Irvine-Gass syndrome is a cystoid macular edema that develops after cataract surgery. Small fluid-filled cavities ("cysts") form within the thickness of the macula, the central area of the retina responsible for fine vision.
It is a rare complication, caused by an inflammatory reaction of the eye following surgery. Most cases remain mild, but the condition can sometimes be more pronounced and significantly impair visual quality.
When does Irvine-Gass syndrome occur?
Irvine-Gass syndrome generally appears a few weeks after cataract surgery, usually around the 1st to 3rd postoperative month. The eye is often painless, with no significant redness, which can surprise patients.
It may affect one eye or both when surgeries are performed close together. Vision may have recovered well in the first few days, then deteriorates secondarily due to the macular edema.
Symptoms of Irvine-Gass syndrome
The most common signs are:
- central blurred vision, at distance and/or near;
- distortion of lines (metamorphopsia): letters or grid patterns appear wavy;
- a sensation of reduced contrast or "washed-out" vision;
- sometimes difficulty reading or driving.
However, peripheral vision is usually preserved. Any unusual decrease in vision after cataract surgery warrants an ophthalmologic examination to rule out Irvine-Gass syndrome or another complication.
Risk factors and causes
The primary cause is an inflammatory reaction of the eye following surgery, leading to increased permeability of retinal capillaries and fluid leakage into the macula.
Known risk factors include:
- complicated cataract surgery (capsular rupture, prolonged manipulation);
- presence of a preexisting epiretinal membrane or vitreomacular traction;
- diabetes or a history of diabetic macular edema;
- known ocular inflammation or uveitis.
Irvine-Gass syndrome can nevertheless occur even after a technically straightforward procedure, in patients with no particular risk factors.
How is the diagnosis made?
The examination begins with visual acuity measurement and a fundus examination. The macula may appear slightly thickened or less transparent, but the appearance can remain subtle to the naked eye.
The gold standard examination is macular OCT, which reveals characteristic cystoid spaces and measures the thickness of the central retina. In some cases, fluorescein angiography may complement the workup to visualize leakage and confirm the diagnosis.
Treatments for Irvine-Gass syndrome
Anti-inflammatory agents and carbonic anhydrase inhibitors
First-line treatment is based on anti-inflammatory eye drops (NSAIDs) and oral carbonic anhydrase inhibitor tablets. This treatment is often combined with corticosteroid eye drops. The goal is to reduce inflammation and promote resolution of the macular edema. The regimen may be more intensive and prolonged than after standard cataract surgery.
Intravitreal injections
If the edema persists despite topical treatment or is significant from the outset, intravitreal injections (most often corticosteroids) may be considered. These injections, performed under sterile conditions, act directly at the macular level to resolve the edema.
Other options and special cases
In rare situations, particularly when associated macular traction is present (epiretinal membrane, significant vitreomacular traction), a vitrectomy with internal limiting membrane peeling may be considered. This indication remains exceptional and is evaluated on a case-by-case basis.
Outcome, prognosis, and follow-up
In the majority of cases, Irvine-Gass syndrome has a favorable outcome: the edema gradually decreases with treatment and vision improves over several weeks to several months. Recovery is often good, although mild persistent visual decrease or contrast difficulties may sometimes remain.
Regular OCT follow-up is important to adjust the duration of treatment and detect rare chronic forms. In diabetic patients or those with other macular diseases, monitoring should be particularly careful.
Practical advice after cataract surgery
After cataract surgery, it is recommended to:
- strictly follow the prescribed postoperative eye drops;
- promptly report any decrease in vision or new distortion of lines;
- not wait for the scheduled follow-up appointment if vision deteriorates suddenly.
Early management of Irvine-Gass syndrome improves the chances of visual recovery and reduces the risk of the edema becoming chronic.
FAQ: Irvine-Gass syndrome
Is Irvine-Gass syndrome common after cataract surgery?
No, it is a rather rare complication. It is a cystoid macular edema caused by a postoperative inflammatory reaction. Most cataract surgeries proceed without Irvine-Gass syndrome, but it can occur even after a technically straightforward procedure, which is why it is important to seek medical advice if vision deteriorates in the weeks following surgery.
When does it most commonly appear?
Irvine-Gass syndrome generally appears a few weeks after cataract surgery, most often between the 1st and 3rd postoperative month. Vision may have recovered well initially, then gradually becomes more blurred as the macular edema develops. The eye is often painless, which can delay consultation.
What symptoms should raise suspicion of Irvine-Gass syndrome?
Typical symptoms include central blurred vision, difficulty reading, a sensation of reduced contrast, and distorted lines (metamorphopsia), occurring after an initial period of improvement. Peripheral vision generally remains preserved. Any unusual decrease in vision after cataract surgery warrants an examination to rule out macular edema or another cause.
What are the causes and risk factors?
The primary cause is postoperative inflammation that increases the permeability of retinal capillaries and leads to fluid leakage into the macula. The risk is higher in cases of complicated surgery (capsular rupture, prolonged manipulation), diabetes, a history of macular edema, uveitis, or the presence of an epiretinal membrane or vitreomacular traction. However, Irvine-Gass syndrome can also occur without any identifiable risk factor.
How is the diagnosis confirmed?
The gold standard examination is macular OCT, which reveals cystoid spaces and measures the thickening of the central retina. The fundus examination may be unremarkable early on, which underscores the value of OCT. In some cases, fluorescein angiography is performed to visualize leakage and support the diagnosis, especially if the course is atypical.
What are the treatments for Irvine-Gass syndrome?
First-line treatment is based on anti-inflammatory eye drops (NSAIDs) often combined with corticosteroid eye drops, with a regimen that is generally more intensive and prolonged than after routine cataract surgery. If the edema is significant or persists, intravitreal injections (anti-VEGF and/or corticosteroids) may be considered to act directly on the macula. More rarely, in cases of associated traction (epiretinal membrane, significant vitreomacular traction), a vitrectomy may be discussed on a case-by-case basis.
How long does it take to recover vision?
Improvement is often gradual over several weeks to several months. In the majority of cases, the edema resolves with treatment and vision improves satisfactorily. However, mild residual difficulties (contrast, fine detail) may persist if the edema was significant or prolonged. The prognosis depends in particular on how quickly treatment is initiated and on the presence of associated factors (diabetes, preexisting macular disease).
Is there a risk that the edema becomes chronic?
Yes, but this remains uncommon. Some forms may persist or recur, particularly in at-risk patients (diabetes, uveitis, macular traction). This is why regular OCT follow-up is important: it allows treatment duration to be adjusted and therapeutic escalation to be proposed if the edema does not resolve sufficiently.
When should you seek prompt medical attention after cataract surgery?
You should seek prompt medical attention if you notice a new decrease in vision, distortion of lines, significant difficulty reading, or a sensation of "washed-out" vision, especially if these symptoms appear some time after the surgery (following an initial phase of improvement). Early management of Irvine-Gass syndrome improves the chances of recovery and reduces the risk of chronicity.
When to consult Julien Gozlan, M.D.?
You may seek a specialist opinion if:
- your vision remains blurred several weeks after cataract surgery;
- you notice wavy lines or image distortion;
- macular edema has been identified on OCT after your surgery.
Julien Gozlan, M.D., ophthalmologist in Paris 16, performs a comprehensive assessment (fundus examination, OCT, and additional imaging if needed), explains the diagnosis of Irvine-Gass syndrome, and proposes a personalized treatment plan.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. sees patients at Paris – Auteuil Ophthalmology Practice for the diagnosis, OCT follow-up, and treatment of Irvine-Gass syndrome (macular edema after cataract surgery).
Book an AppointmentFurther reading
- Cataract surgery: procedure, implants, and recovery.
- Macular OCT: the key examination for analyzing macular edema.
- Intravitreal injections: role in the treatment of macular edema.
- Diabetic macular edema: another common cause of macular edema.