
Diabetic macular edema is a common complication of diabetes that affects the macula, the central portion of the retina responsible for fine vision. It causes blurred and distorted vision. Julien Gozlan, M.D., ophthalmologist at the Paris – Auteuil Ophthalmology Practice, provides a clear explanation of the causes, diagnosis by macular OCT, and modern treatments for diabetic macular edema.
What is diabetic macular edema?
Diabetic macular edema (DME) refers to an accumulation of fluid within the central retina. Weakened capillaries leak, the macula thickens, and central vision becomes blurred. This complication can occur at any stage of diabetic retinopathy, sometimes very early on.
Symptoms: when should you seek medical advice?
The most common signs include blurred central vision, wavy lines (metamorphopsia), faded colors, and difficulty reading. In a diabetic patient, these symptoms should raise suspicion of diabetic macular edema and prompt a rapid consultation, including a macular OCT scan.
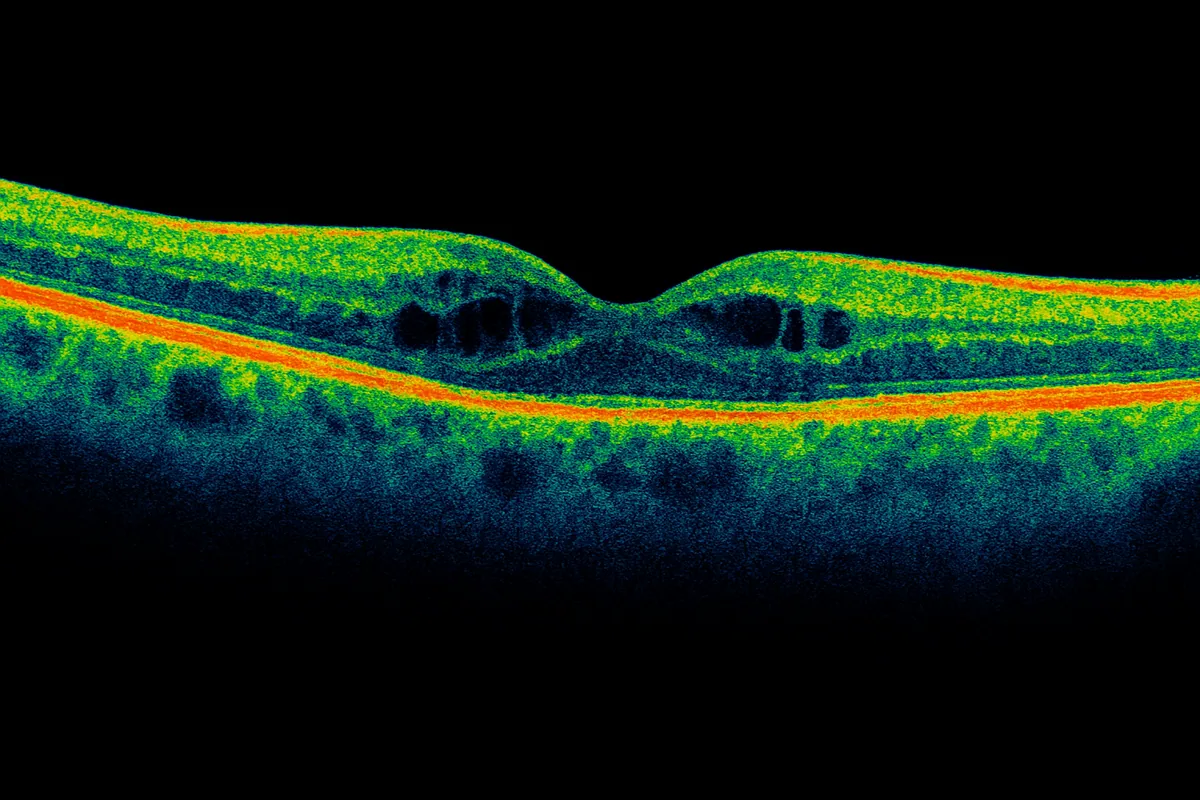
How is the diagnosis confirmed?
The key examination is macular OCT, which reveals thickening and typical intraretinal "cysts." In some cases, fluorescein angiography helps locate the leakage sites. A fundus examination completes the evaluation and looks for other signs of diabetic retinopathy.
Causes and risk factors
Diabetic macular edema is mainly caused by chronic poor glycemic control. Duration of diabetes, high blood pressure, hypercholesterolemia, and smoking increase the risk. Improving these parameters reduces the onset and severity of the disease and protects the macula in the long term.
Treatments for diabetic macular edema
Anti-VEGF intravitreal injections
As the first-line treatment, anti-VEGF intravitreal injections reduce vascular leakage and dry up diabetic macular edema. After an initial monthly loading phase, the frequency is personalized (treat and extend) based on vision and OCT findings.
Corticosteroid intravitreal injections
In certain cases, when the response is insufficient or inflammation is present, a sustained-release corticosteroid implant can stabilize diabetic macular edema. Intraocular pressure monitoring is then required, as with other intravitreal injection treatments.
Focal macular laser
Laser treatment can complement injections by sealing localized leaks. Painless, it helps control DME when the responsible areas are clearly identified on angiography and macular OCT.
Overall metabolic control and follow-up
Treatment effectiveness also depends on good diabetes control (glycated hemoglobin or HbA1c), management of high blood pressure and lipid levels, and smoking cessation. These measures reduce the risk of diabetic macular edema and improve visual stability. For additional information on daily diabetes management, you may also visit the French Diabetes Federation.
Prognosis and follow-up schedule
When detected early, diabetic macular edema most often stabilizes and can improve. The number of intravitreal injections varies from patient to patient. Regular monitoring with OCT and visual acuity measurements guides treatment frequency in order to maintain the best possible daily vision.
Practical tips to limit recurrences
Monitor your vision at home (for example with an Amsler grid), one eye at a time, and seek urgent medical attention in case of sudden vision loss, a central dark spot, or significant distortion. Keep a log of your injections (dates, treated eye) and plan your appointments ahead. Regarding lifestyle: aim for the glycated hemoglobin (HbA1c) target set by your diabetologist, control your blood pressure and cholesterol, maintain a balanced diet, and quit smoking. These habits enhance the effects of treatment.
FAQ: frequently asked questions about diabetic macular edema
Can diabetic macular edema resolve without treatment?
Diabetic macular edema may fluctuate with diabetes control and blood pressure management, but a complete and lasting resolution without specific treatment remains uncommon when the edema is well established. In practice, intravitreal injections and sometimes laser are often necessary to protect the macula. Relying solely on overall metabolic control wastes precious time for central vision, especially if visual decline is already noticeable or if OCT shows significant edema.
At what stage should intravitreal injections be started?
The decision is not based solely on visual acuity measurements. It takes into account the patient's perceived impairment (reading, driving, screen work), macular thickness on OCT, and the appearance of the retina (significant leakage, cysts, involvement of one or both eyes). Mild edema in a minimally symptomatic patient may sometimes be monitored closely, whereas more pronounced or rapidly progressive edema warrants early intravitreal injections to limit long-term vision loss. The strategy is therefore personalized after a comprehensive examination.
Will I still be able to drive and work with diabetic macular edema?
Many patients maintain sufficient vision for daily activities, especially if the other eye sees well and the edema is treated promptly. Driving and working remain possible as long as vision meets the legal and safety requirements. However, certain visually demanding occupations (professional driving, precision work, monitoring multiple screens) may require temporary adjustments. Your ophthalmologist assesses on a case-by-case basis the compatibility between your vision, your treatment, and your professional activity or regular vehicle driving.
Are injections for diabetic macular edema needed for a long time?
In most cases, this is not a "one-time" treatment. After a few closely spaced intravitreal injections, the frequency is adjusted based on macular OCT findings and visual stability. In some patients, intervals can be gradually extended to several months, or even temporarily suspended if the edema remains quiescent. In others, long-term monitoring with occasional injections remains necessary. The goal is to adjust the number of injections to the strict minimum needed to keep the macula as dry as possible, while minimizing the burden on the patient.
Can good diabetes control reduce the number of injections?
Yes, better glycemic control (HbA1c close to the target set with your diabetologist), combined with well-managed blood pressure and cholesterol levels, helps stabilize the retina. This does not replace ocular treatments but often helps reduce the frequency of edema flare-ups and, in the long term, the number of injections required. In practice, the best outcomes are seen in patients who combine rigorous ophthalmologic follow-up, consistent injection treatment, and serious overall management of their diabetes and cardiovascular risk factors.
Does diabetic macular edema affect both eyes equally?
Both eyes are not always affected at the same time or with the same severity. Some patients develop diabetic macular edema in only one eye for several years, while others see edema appear in the second eye sooner. This is why, even if only one eye is being treated, the other must be monitored regularly with fundus examination and OCT. The advantage of early diagnosis in the still-unaffected eye is the ability to start treatment before significant visual loss occurs.
What are the differences compared to macular edema from other causes (vein occlusion, surgery, etc.)?
Diabetic macular edema occurs within the context of diabetic retinopathy and a chronic systemic disease. Its treatment must therefore always take into account the underlying diabetes and overall vascular health. In contrast, macular edema following venous occlusion, surgery, or other inflammatory conditions does not involve the same mechanisms and is not associated with the same systemic risks. OCT images may look similar, but the clinical context, type of follow-up, and sometimes the choice of treatment (type of drug, monitoring schedule) are not entirely the same. This underscores the importance of an accurate diagnosis and a personalized strategy for each patient.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. offers a comprehensive evaluation and a personalized treatment plan for diabetic macular edema: macular OCT, intravitreal injections, and regular follow-up.
Book an AppointmentFurther reading
- Diabetic retinopathy: understanding the lesions and prevention.
- Intravitreal injections: procedure, efficacy, and follow-up.