
A retinal tear is a break in the retinal tissue, often caused by traction from the vitreous (the gel that fills the eye). It can remain silent for a long time or present with floaters, flashes of light, or a curtain effect in the visual field. The main risk is progression to a retinal detachment, which constitutes a surgical emergency. Dr Julien Gozlan, ophthalmologist in Paris 16, explains the warning symptoms, diagnosis, laser treatments, and the follow-up that should be implemented.
What is a retinal tear?
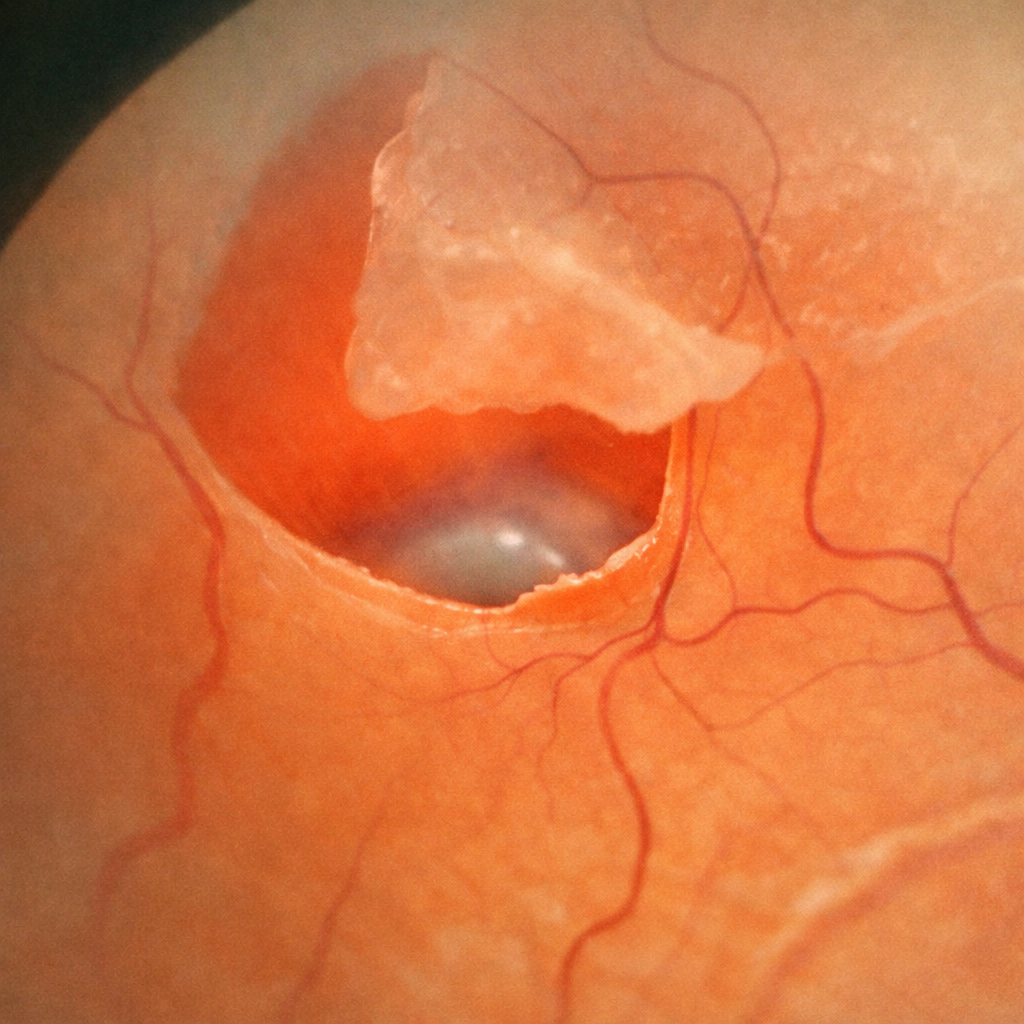
The retina is a thin membrane that lines the back of the eye and converts light into nerve signals. With age, the vitreous liquefies and can separate from the retina (known as posterior vitreous detachment). If the traction is significant at certain attachment points, it can create a retinal tear.
The main types include:
- horseshoe tears, caused by strong vitreous traction;
- retinal holes (often in highly myopic patients);
- tears in degenerative areas of the peripheral retina.
Not all retinal tears lead to retinal detachment, but any significant tear must be evaluated promptly to determine whether preventive treatment is needed.
Symptoms: when should a retinal tear be suspected?
A retinal tear can be completely asymptomatic, but several signs should raise concern, especially if they are recent and unilateral (affecting one eye only):
- sudden onset of numerous or unusual-looking floaters;
- perception of flashes of light in the dark or with eyes closed;
- impression of a shower of soot or multiple small dark spots;
- onset of a dark curtain or a blocked area in part of the visual field.
These symptoms do not always indicate a retinal tear or retinal detachment, but they warrant a prompt ophthalmological consultation, ideally within 24 to 48 hours, to assess the condition of the retina.
Diagnosis: how is a retinal tear examined?
The diagnosis of a retinal tear is based on a comprehensive dilated fundus examination. The ophthalmologist looks for:
- the presence of a tear or a retinal hole;
- predisposing peripheral degenerations (lattice degeneration, snail-track degeneration, etc.);
- signs of early retinal detachment (elevation of the retina around the tear);
- hemorrhages or exudates in the vitreous.
Depending on the context, additional imaging studies may be used:
- macular OCT to analyze the central retina if vision is decreased;
- ocular ultrasound in cases of media opacity (vitreous hemorrhage, dense cataract);
- an examination with scleral indentation to visualize difficult-to-access peripheral retina.
The objective is twofold: to confirm the retinal tear, specify its type and location, and to look for any associated detachment.
Causes and risk factors
Several situations increase the risk of retinal tears:
- High myopia (longer eye, more stretched and fragile retina);
- Recent posterior vitreous detachment with significant traction;
- History of retinal detachment or tear in the fellow eye;
- Family history of retinal detachment;
- Ocular trauma (direct blow, sports ball, airbag);
- certain ocular surgeries (for example after cataract surgery or vitrectomy, depending on the context);
- presence of known peripheral retinal degenerations.
In at-risk patients, regular fundus examinations allow early detection of abnormalities and preventive treatment when necessary.
How is a retinal tear treated?
Pupil dilation and positioning
Mydriatic eye drops are instilled to dilate the pupil and allow a full examination of the fundus. After 20–30 minutes, the patient sits at the slit lamp with chin on the rest, and a contact lens is applied to the eye.
Laser photocoagulation around the tear
The ophthalmologist applies multiple laser impacts around the tear under topical anaesthesia (eye drops). These impacts create a circular scar barrier that seals the retina to the eye wall and prevents detachment. The session lasts a few minutes. Cryotherapy may be performed instead of or in addition to laser when fundus visibility is poor.
Follow-up and review
A fundus check is performed 1 to 2 weeks after laser to confirm the strength of the scar barrier. If new symptoms appear (visual loss, dark curtain, increase in floaters), urgent consultation is required.
Prognosis and follow-up after treatment
After laser or cryotherapy treatment, healing takes several days to consolidate. During this period, any new symptoms (sudden increase in floaters, appearance of a curtain or missing area in the visual field) should prompt an immediate follow-up visit.
The prognosis is generally favorable when the tear is treated in time, before any retinal detachment occurs. Follow-up includes:
- a close follow-up examination after laser treatment (usually within the following weeks);
- longer-term monitoring, especially in cases of high myopia or personal/family history;
- clear explanation of warning signs that should never be ignored.
Even after successful treatment, new tears may develop elsewhere on the retina. This underscores the importance of remaining alert to symptoms and maintaining regular follow-up.
Practical advice for patients
In practice, if a retinal tear has been suspected or confirmed:
- do not delay seeking consultation if you experience floaters, flashes, or a visual curtain;
- attend all follow-up appointments and follow recommendations after laser or surgery;
- avoid violent impacts to the head or contact sports in the days following treatment;
- seek emergency consultation if a fixed shadow or black curtain appears in the visual field;
- inform your ophthalmologist of any planned ocular surgery or recent ocular trauma.
FAQ: Retinal tears
Is a retinal tear an emergency?
A retinal tear is not always a life-threatening emergency, but it constitutes a relative ophthalmological emergency, as it can precede a retinal detachment. In the presence of unusual floaters, flashes of light, or a curtain in the visual field, it is recommended to seek prompt consultation, ideally within 24 to 48 hours, to assess the condition of the retina and provide treatment if necessary.
Is laser treatment for a retinal tear painful?
Retinal laser treatment is performed under topical anesthesia with eye drops. It may be felt as discomfort or irritation, sometimes with brief mild pain during certain laser spots, but it is generally tolerable. A feeling of eye fatigue or irritation is possible after the session and resolves with the prescribed eye drops. If significant or persistent pain occurs, the office should be contacted.
Do all retinal tears lead to detachment?
No. Some retinal tears remain stable, especially when they are small, longstanding, or already surrounded by a natural scar. However, a fresh tear that is poorly delimited or highly tractional has a real risk of leading to retinal detachment if left untreated. This is why the ophthalmologist evaluates the size, location, and appearance of each tear before deciding whether to recommend preventive laser treatment.
Can I travel by plane after treatment for a retinal tear?
After laser treatment alone, air travel is generally possible once the eye has stabilized, unless the ophthalmologist advises otherwise. However, if a vitrectomy with intraocular gas has been performed, air travel is strictly contraindicated as long as the gas is present, due to the risk of a dangerous increase in intraocular pressure. The surgeon always specifies the duration during which flying is prohibited and the date from which air travel is permitted again.
What signs should prompt an emergency consultation after laser treatment for a tear?
After laser treatment, you should seek emergency consultation if the following occur: a sudden decrease in vision, a black curtain or fixed shadow in the visual field, a sudden increase in floaters or flashes of light, or significant pain. These signs may suggest a retinal detachment or a new tear, which require prompt reassessment. When in doubt, it is better to contact the office than to wait for the scheduled follow-up.
Can I resume sports after a retinal tear?
Yes, in most cases, but with precautions. Gentle physical activities (walking, leisurely cycling) can be resumed quickly with the ophthalmologist's approval. However, contact sports (boxing, martial arts, rugby) or activities with a risk of head impact should be discussed on a case-by-case basis, especially in highly myopic patients or those with a history of retinal detachment. The goal is to limit trauma that could reactivate traction on the retina.
Once treated, can a retinal tear "come back"?
A tear that has been properly surrounded by laser is generally permanently healed. It does not "close up," but the retina is welded around the weakened area, which protects against the progression of subretinal fluid. However, new tears may appear later at a different location on the retina, especially in at-risk individuals. This highlights the importance of regular follow-up and vigilance regarding new symptoms.
Am I at greater risk of retinal detachment if a family member has had surgery for it?
Yes, a family history of retinal detachment is one of the risk factors, especially when combined with high myopia. This does not mean detachment is inevitable, but it warrants closer monitoring of the fundus and prompt consultation if symptoms arise (floaters, flashes, curtain effect). The ophthalmologist may also decide to protect certain vulnerable areas with preventive laser in well-defined cases.
When to consult Dr Julien Gozlan?
You should seek an urgent consultation if you experience unusual floaters, flashes of light, or the onset of a curtain in the visual field. A check-up is also recommended if you are highly myopic, if you have a personal or family history of retinal detachment, or if a tear has already been treated in the fellow eye.
Dr Julien Gozlan, ophthalmologist in Paris 16, performs a thorough fundus examination, supplemented if needed with imaging studies, and discusses with you the need for laser treatment, close surveillance alone, or possible surgical management in cases of early detachment.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan welcomes you at the Paris – Auteuil Ophthalmology Practice to evaluate a retinal tear, screen for any at-risk peripheral lesions, and implement, if needed, preventive laser treatment or a personalized follow-up plan.
Book an AppointmentFurther reading
- Retinal detachment: emergency symptoms and surgical management.
- Macular OCT: an essential imaging examination for analyzing the retina.
- Intravitreal injections (IVT): associated treatments for certain retinal conditions.
- Retinal tear: urgent laser treatment : emergency management by laser photocoagulation.