
Choroidal metastasis refers to a secondary tumor located in the choroid, the vascular membrane situated between the retina and the sclera of the eye. Dr Julien Gozlan, an ophthalmologist specializing in retina surgery in Paris 16, manages patients presenting with this ocular condition, which is often the first sign of a distant cancer. This article details the mechanisms of choroidal metastasis, the symptoms that should raise concern, the essential diagnostic examinations, and current treatment options, in a reassuring and educational approach.
What is choroidal metastasis?
The choroid is the most vascularized tissue in the eye. This abundance of blood vessels makes it a favorable site for the implantation of circulating cancer cells originating from a primary tumor located elsewhere in the body. Choroidal metastasis is thus the most common intraocular malignant tumor in adults, ahead of choroidal melanoma, which is a primary tumor of the eye.
The cancers that most frequently metastasize to the choroid are breast cancer in women and lung cancer in men. Other primary sites are possible: kidney, gastrointestinal tract, thyroid, or prostate cancers. In approximately 30% of cases, choroidal metastasis constitutes the first sign of a previously unknown cancer, underscoring the importance of a rapid and accurate ophthalmological diagnosis.
Causes and risk factors of choroidal metastasis
The occurrence of choroidal metastasis is directly linked to the hematogenous spread (via the bloodstream) of tumor cells. The risk factors are therefore those of the primary cancer itself. Certain elements increase the likelihood of ocular involvement:
- Metastatic breast cancer: responsible for approximately 40 to 50% of choroidal metastases.
- Bronchopulmonary cancer: the second most common cause, often diagnosed at an advanced stage.
- Advanced stage of cancer disease: the presence of metastases in other organs (bone, liver, brain) increases the risk of choroidal involvement.
- Lack of regular oncological follow-up: delaying the detection of secondary localizations.
It is important to note that choroidal metastasis can be unilateral or bilateral, and multiple lesions may be observed in the same eye. Systematic fundus examination in cancer patients is therefore essential.
Symptoms and diagnosis of choroidal metastasis
Suggestive symptoms
The clinical signs depend on the size and location of the tumor within the choroid. The most common symptoms are:
- Vision loss: progressive or sudden, especially if the lesion is close to the macula.
- Perception of dark spots or blurry areas in the visual field (scotoma).
- Image distortion (metamorphopsia), similar to what can be observed in age-related macular degeneration (AMD).
- Sensation of flashes of light or the appearance of floaters.
- Sometimes, choroidal metastasis is entirely asymptomatic and discovered during a routine examination.
Diagnostic examinations
The diagnosis relies on a set of complementary examinations performed at Dr Julien Gozlan's practice:
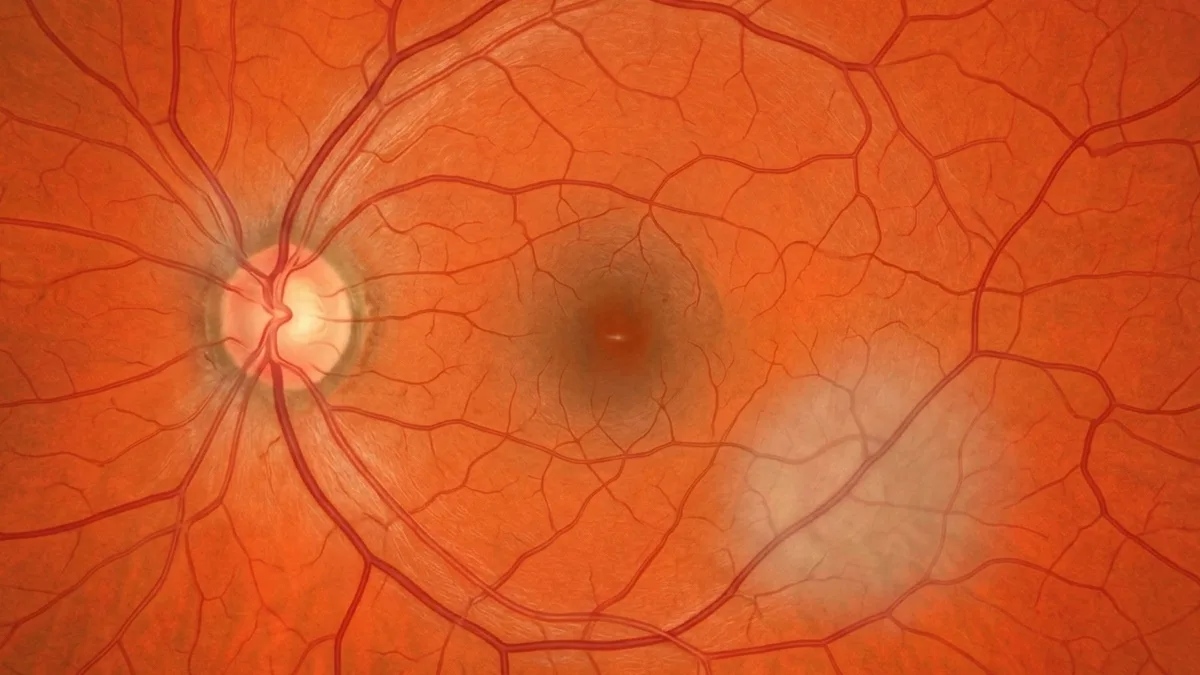
- Fundus examination: this typically reveals a yellowish, flat lesion, often accompanied by a serous retinal detachment.
- OCT (optical coherence tomography): this non-invasive examination allows analysis of the retinal layers and visualization of the serous detachment associated with choroidal metastasis.
- Fluorescein angiography: this highlights the vascular abnormalities of the lesion and guides the differential diagnosis.
- B-scan ocular ultrasound: this measures the thickness of the tumor and assesses its extent.
- OCT angiography: a valuable supplementary examination for analyzing tumor vascularization without contrast injection.
These examinations allow choroidal metastasis to be distinguished from other conditions such as choroidal melanoma, choroidal hemangioma, or central serous chorioretinopathy. A complete oncological staging workup is systematically coordinated with the oncology team.
Treatment and management of choroidal metastasis
The management of choroidal metastasis is multidisciplinary, involving the ophthalmologist specializing in the retina and the oncologist. The choice of treatment depends on several factors: the size and number of lesions, the type of primary cancer, the patient's general condition, and the response to systemic treatments.
Systemic treatments
Chemotherapy, hormone therapy (particularly in breast cancer), targeted therapies, and immunotherapy form the cornerstone of treatment. These treatments act on all metastatic sites, including choroidal metastasis. Significant regression of the ocular lesion is often observed with appropriate systemic treatment.
Local treatments
When choroidal metastasis is large, threatens central vision, or is resistant to systemic treatment, local treatments may be proposed:
- External beam radiotherapy: focused irradiation of the choroidal tumor, effective in reducing the size of the lesion.
- Proton therapy: a high-precision radiotherapy technique, particularly suited to ocular tumors.
- Brachytherapy (radioactive plaque): application of a radioactive disc in contact with the sclera overlying the tumor.
- Intravitreal injections (IVT): in certain cases, intravitreal injections of anti-VEGF agents may be used to treat associated serous retinal detachment.
Dr Julien Gozlan provides close ophthalmological monitoring of choroidal metastasis under treatment, with regular examinations (OCT, fundus examination, ultrasound) to assess the therapeutic response and adjust management accordingly.
Visual prognosis and follow-up
The visual prognosis of a choroidal metastasis depends primarily on its location relative to the macula and on the speed of treatment. Peripheral lesions, detected early, often allow satisfactory functional vision to be preserved. Conversely, direct macular involvement or extensive exudative retinal detachment can lead to more severe vision loss.
Regular follow-up with OCT and fundus examination is essential to detect any recurrence or the appearance of new lesions. The overall prognosis is also linked to the progression of the primary cancer. Close dialogue between the ophthalmologist and the oncologist helps optimise the patient's overall management.
FAQ: choroidal metastasis
Is choroidal metastasis painful?
As a general rule, choroidal metastasis is not painful. Symptoms are essentially visual: reduced vision, spots in the visual field, or image distortion. Ocular pain may, however, occur in cases of associated secondary glaucoma, but this complication remains rare. An ophthalmological examination allows for a rapid assessment.
Can one have a choroidal metastasis without a known cancer?
Yes, in approximately 30% of cases, choroidal metastasis is the first sign of a cancer that has not yet been diagnosed. This is why the discovery of a suspicious lesion during fundus examination systematically triggers a complete oncological work-up to identify the primary tumour. Early diagnosis is critical for prognosis.
What examinations are performed to diagnose a choroidal metastasis?
Diagnosis is based on fundus examination, OCT, fluorescein angiography, B-mode ocular ultrasound, and sometimes OCT-angiography. These examinations are performed at Dr Julien Gozlan's practice. They make it possible to characterise the lesion, measure it, and distinguish it from other ocular tumours such as choroidal melanoma.
Is treatment for choroidal metastasis effective?
In the majority of cases, systemic treatments (chemotherapy, hormone therapy, immunotherapy) allow regression of the choroidal metastasis. Local treatments such as radiotherapy complement management when necessary. The response to treatment is monitored through regular examinations, and many patients retain useful vision.
Is ophthalmological follow-up necessary after treatment?
Absolutely. Close ophthalmological follow-up is essential to assess the response to treatment, detect any possible recurrence of the choroidal metastasis, or the appearance of new lesions. The frequency of consultations is tailored to each patient, in coordination with the oncology team. Dr Julien Gozlan provides this personalised follow-up.
Can a choroidal metastasis cause retinal detachment?
Yes, choroidal metastasis can cause exudative retinal detachment (accumulation of fluid beneath the retina) due to disruption of the choroidal vascular barrier. This type of detachment differs from classic rhegmatogenous retinal detachment and is treated primarily by targeting the tumour itself. Dr Julien Gozlan assesses this complication precisely using OCT and ultrasound.
When should you consult Dr Julien Gozlan?
Any unexplained loss of vision, appearance of spots or visual distortions in a patient being treated for cancer — or even in the absence of any known condition — should prompt an urgent ophthalmological consultation. Dr Julien Gozlan, a retinal specialist in Paris 16, has all the necessary diagnostic equipment (OCT, OCT-angiography, angiography, ultrasound) to confirm or rule out a choroidal metastasis and to coordinate management with the oncology team without delay.
📍 Consultation at the Cabinet Ophtalmologique Paris – Auteuil
Dr Julien Gozlan sees patients at the Cabinet Ophtalmologique Paris – Auteuil for the diagnosis and follow-up of choroidal metastases. With a comprehensive technical platform and recognised expertise in retinal pathology, he accompanies you with rigour and care at every stage of your management.
Book an Appointment on DoctolibFurther reading
- OCT (optical coherence tomography): discover this key examination for analysing retinal layers and monitoring macular conditions.
- OCT-angiography: a non-invasive examination enabling visualisation of retinal and choroidal vasculature without injection.
- Fluorescein angiography: understanding the procedure and the value of this examination in diagnosing fundus pathologies.
- Intravitreal injections (IVT): indications, procedure, and follow-up for this commonly used treatment in retinal pathology.