
Age-related macular degeneration (AMD) is a disease affecting the central part of the retina, known as the macula. It mainly affects people over the age of 55–60 and can lead to central vision loss. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, provides a clear explanation of what age-related macular degeneration (AMD) is, its forms, symptoms, and available treatments.
Overview: what is the macula?
The retina lines the back of the eye and acts as a "film" or image sensor. At its center lies a small, highly specialized area: the macula.
It is responsible for sharp central vision, reading, recognizing faces, and perceiving fine details. When this area is affected by age-related macular degeneration (AMD), central vision is impaired, while peripheral vision (side vision) generally remains intact.
Age-related macular degeneration: a disease of central retinal aging
Age-related macular degeneration corresponds to abnormal aging of the macula. It is the leading cause of low vision in adults in industrialized countries.
The exact cause of AMD is not fully understood, but several factors are involved:
- age (the main risk factor);
- smoking, which significantly increases the risk;
- family history of the same disease;
- certain cardiovascular factors (hypertension, cholesterol, diabetes);
- possible environmental factors (diet, sun exposure, etc.).
There is an early form, followed by two advanced forms of age-related macular degeneration: a dry (atrophic) form and a wet (exudative) form.
The early form: age-related maculopathy
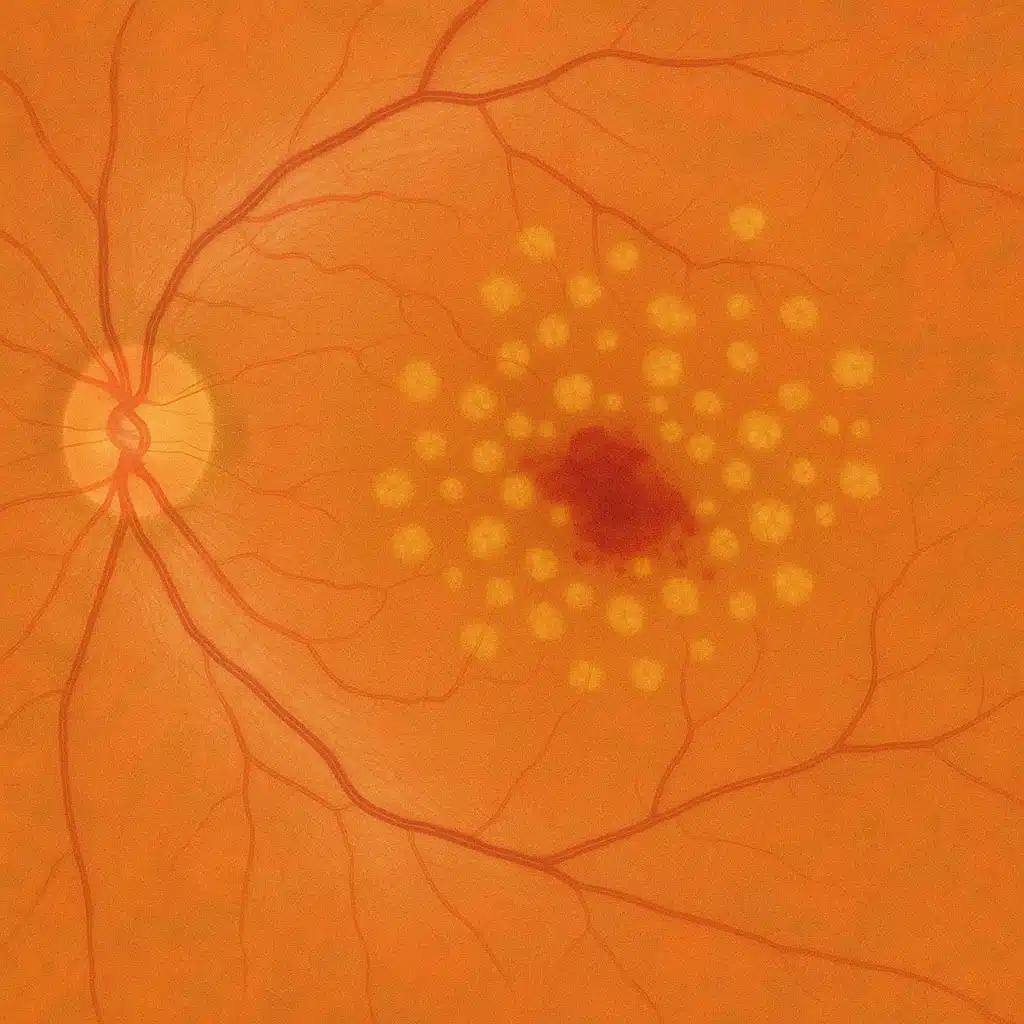
In the early stage of AMD, small yellowish deposits called drusen accumulate beneath the macula. They are visible on fundus examination and on retinal OCT (retinal imaging).
At this stage:
- vision may be normal or only minimally affected;
- there are often no noticeable symptoms;
- this is referred to as age-related maculopathy rather than advanced AMD.
The main objective at this stage is regular monitoring, in order to promptly detect any progression toward the atrophic or exudative form of age-related macular degeneration.
Atrophic (dry) form
In the atrophic form of AMD, the macula gradually thins: the visual cells progressively disappear.
The consequences are:
- a slow and progressive decline in central vision;
- difficulty reading, even with appropriate glasses;
- sometimes a blurry spot in the center of the visual field.
Currently, there is no recognized curative treatment for this form of age-related macular degeneration. Management is based on:
- adapting lighting and using visual aids (magnifiers, magnifying systems);
- low vision rehabilitation;
- addressing risk factors (smoking, blood pressure, cholesterol, etc.).
Regular ophthalmological follow-up remains essential, as the condition may evolve over time.
Exudative (wet) form: a medical emergency
In the exudative form of age-related macular degeneration, abnormal blood vessels grow beneath or within the central retina. These vessels are fragile and leak fluid or blood, causing detachments and hemorrhages.
This condition often leads to rapid vision loss:
- distortion of straight lines (they appear wavy);
- a dark or blurry spot in the center of vision;
- a sensation of a central "hole";
- sudden vision loss in one eye.
This is an ophthalmological emergency: it is important to see a specialist promptly to confirm the diagnosis (fundus examination, OCT, sometimes angiography) and begin treatment without delay.
What treatments are available?
Intraocular injections for the exudative form
The standard treatment for the exudative form of AMD relies on intraocular injections of medications called anti-VEGF agents. They are injected into the eye, into the vitreous cavity, in the office or in a dedicated procedure room.
These medications:
- inhibit the growth of abnormal blood vessels;
- reduce fluid leakage and hemorrhages;
- most often help to stabilize vision, and sometimes improve it.
The injections are generally administered on a repeated basis (several times per year), following a protocol tailored to each patient, based on the progression observed on OCT.
General measures and screening
For all individuals affected by or at risk of age-related macular degeneration, the following recommendations apply:
- complete smoking cessation;
- good cardiovascular health practices (blood pressure, cholesterol, diabetes management);
- a balanced diet rich in fruits, vegetables, and oily fish;
- regular ophthalmological follow-up, even in the absence of symptoms.
Several risk factors can be addressed on a daily basis, such as quitting smoking or adapting one's diet, particularly in patients who already have risk factors for AMD.
An Amsler grid (a grid pattern) can be used at home to monitor the appearance of distortions in the center of the visual field and to seek prompt medical advice if any changes occur.
Frequently asked questions about age-related macular degeneration (AMD)
Does AMD inevitably lead to blindness?
AMD almost never causes total blindness, as peripheral vision is generally preserved. However, it can significantly reduce central vision, making reading, face recognition, or driving difficult. The goal of monitoring and treatment is to slow the progression and preserve functional central vision for as long as possible, while learning to make the best use of peripheral vision if needed.
Is AMD always hereditary?
There are genetic susceptibility factors for AMD: having a close relative affected increases the risk of developing the disease. However, heredity does not explain everything. Age, smoking, certain cardiovascular factors (blood pressure, cholesterol, obesity), and lifestyle play a major role. It is therefore possible to be affected without any family history, and conversely, one may never develop AMD despite a genetic predisposition.
Can AMD be prevented or delayed through diet?
No diet can completely prevent the onset of AMD, but certain habits can help slow its progression. A diet rich in colorful fruits and vegetables (lutein, zeaxanthin), oily fish (omega-3 fatty acids), and low in tobacco and excessive alcohol consumption is recommended. In very specific profiles, your ophthalmologist may discuss specific dietary supplements, but these do not replace follow-up care or prescribed treatments.
Does AMD affect one eye or both?
AMD is a disease that generally affects both eyes, but often at different stages. It is not uncommon for only one eye to be symptomatic at first, with the other compensating for the vision loss. This is one of the reasons why a comprehensive ophthalmological examination of both eyes is essential, even if you feel that everything is fine on the unaffected side. Regular follow-up helps detect early involvement of the second eye.
How can I monitor AMD progression at home?
In addition to clinical follow-up, it is helpful to regularly test each eye separately by looking at text or an Amsler grid: look for the appearance of wavy lines, missing letters, or a central spot. You should also be alert to any impression of rapid vision loss on one side. If any unusual change occurs, it is recommended to seek medical advice without delay, even if your next check-up appointment is already scheduled.
Can I continue driving if I have AMD?
The ability to drive depends on the level of visual acuity and the quality of vision in each eye. Some early or moderate forms allow driving that is still compatible with regulations, sometimes with appropriate corrective lenses. However, if central vision becomes too impaired, driving can become dangerous and is no longer permitted. This question should be discussed on a case-by-case basis with your ophthalmologist, who will advise you based on your examination results and current legislation.
How often should I have check-ups if I have AMD or am at high risk?
The frequency of follow-up depends on the stage of the disease and the type of AMD. In the presence of simple drusen without symptoms, an annual consultation may be sufficient, unless new symptoms appear. In cases of confirmed AMD, follow-up is more frequent, with regular imaging examinations (OCT in particular). After an episode of exudative AMD treated with injections, check-ups are often scheduled every 1 to 3 months initially, then spaced out depending on stability. Your ophthalmologist will establish a schedule tailored to your situation.
When should you see Julien Gozlan, M.D.?
You should seek prompt consultation if you notice:
- a sudden drop in vision in one eye;
- straight lines appearing wavy;
- a dark or blurry spot in the center of your vision;
- or if you have already been told about a macular condition or possible AMD requiring monitoring.
📍 AMD consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. sees patients at Paris – Auteuil Ophthalmology Practice for the screening, monitoring, and treatment of age-related macular degeneration (AMD).
Book an AppointmentFurther reading
- Retinal OCT: an essential imaging examination for analyzing the macula.
- Intravitreal injections: practical details of injections for this disease.
- AMD self-monitoring: how to use the Amsler grid?