
A macular hole is a small opening in the center of the retina, in the macula. This condition often causes a decrease in central vision, a spot in the middle of the image, and distorted lines. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, explains the diagnosis by OCT, treatment, and prognosis.
What is a macular hole?
A macular hole is a more or less complete disruption of the retinal layers at the center of the macula. It most often affects only one eye. The patient may describe blurred central vision, difficulty reading, or the sensation that a small "spot" is missing in the image.
There are several stages: initially, vitreous traction can distort the fovea; then the opening can widen and become full-thickness. The size and duration are important factors for visual recovery.
Why does this lesion occur?
The main cause is vitreomacular traction. With age, the vitreous gel liquefies and progressively detaches; if it remains attached to the fovea, it can pull on the macula and create the opening. More rarely, this problem occurs after trauma, in high myopia, or in association with an epiretinal membrane.
Symptoms: when should you seek medical advice?
The signs are often progressive and become bothersome for precision activities:
- decreased visual acuity at distance and/or near;
- metamorphopsia: straight lines appear wavy;
- central scotoma: a small dark or blurry spot in the center;
- sometimes monocular diplopia.
If these symptoms have appeared recently, a prompt ophthalmological consultation is recommended to confirm the diagnosis and prevent worsening.
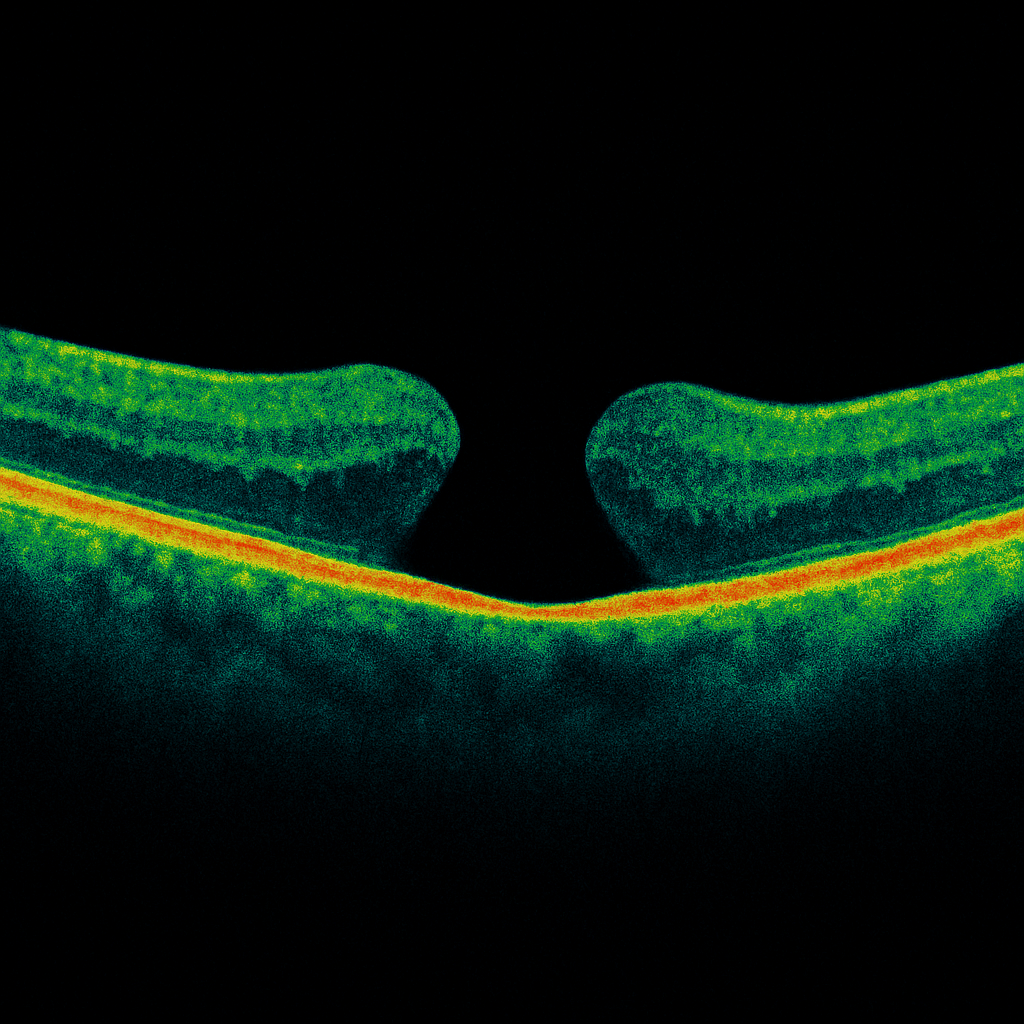
Diagnosis: macular OCT, the key examination
Macular OCT is the gold standard examination. It visualizes the retinal structure in cross-section, precisely measures the size of the opening, and determines the stage of the macular hole. It also helps identify persistent traction, an associated membrane, or thickening of the edges.
An OCT is also useful for detecting associated conditions (AMD, edema, myopic damage), as the final visual outcome also depends on the condition of the outer retinal layers.
Typical OCT findings and prognosis
OCT provides useful prognostic criteria before surgery, including:
- minimum diameter and base diameter;
- persistent vitreous adhesion and tangential traction;
- cuff of edema and perifoveal thickening;
- integrity of the ellipsoid zone and the external limiting membrane (outer layers).
The more recent and smaller the lesion, the greater the chance of significant visual improvement after closure.
Treatment: vitrectomy and peeling
The treatment of a macular hole is surgical and relies on a vitrectomy. The vitreous is removed, then the surgeon performs internal limiting membrane peeling to release traction and help the macula close. A gas injection is performed at the end of the procedure to keep the central area in proper position during healing.
Postoperative course: positioning, gas, and precautions
After surgery, a face-down positioning may be recommended for a few days, depending on the size and context. Vision remains blurry as long as the gas is present, then gradually improves as the gas resorbs.
Air travel and high altitude are strictly prohibited as long as the gas bubble persists, as it can expand and cause a severe increase in intraocular pressure.
When should surgery be performed?
In practice, surgery is often recommended as soon as the diagnosis is confirmed, because a macular hole tends to enlarge over time. Early management increases the chances of closure and optimizes the prognosis.
FAQ: frequently asked questions about macular holes
Can a macular hole heal on its own?
A full-thickness macular hole rarely closes spontaneously. In most cases, when it is well-established and confirmed by OCT, vitrectomy with membrane peeling remains the standard treatment to achieve anatomical closure and improvement in central vision.
Is surgery an emergency?
It is not an "immediate" emergency, but it is best not to wait too long. The size of the macular hole and its duration influence visual recovery: the earlier the treatment, the better the chances of regaining functional central vision for reading and precision tasks.
How long does the gas bubble last?
The lifespan of the bubble depends on the type of gas used and its concentration. In practice, it remains in place for approximately 2 to 8 weeks. During this period, vision is very blurry or partially obscured, then gradually clears as the gas resorbs and is replaced by the eye's natural fluid.
Can I drive after the surgery?
Driving is only permitted when vision is deemed adequate by your ophthalmologist, and only after the gas has completely resorbed. Recovery also depends on which eye was operated on (dominant eye or not), the vision in the other eye, and the visual demands related to your activity (short trips, highway driving, night driving, etc.).
When can I return to work?
Returning to work depends on the type of work (screen use, fine manipulation, heavy lifting, travel) and the possible need for prolonged positioning during the first few days. Sedentary work can sometimes be resumed within a few days or weeks, while physical activity or work with a risk of eye injury will require a longer delay. The timeline is tailored on a case-by-case basis during postoperative consultations.
Can I resume sports?
Contact sports, intense exertion, and activities involving jarring movements (running, jumping, racket sports) are generally postponed for several weeks, especially when a gas bubble is present or the retina is fragile. Gentle activities such as walking can often be resumed sooner, according to your surgeon's specific recommendations.
Can I fly after the procedure?
No, as long as the gas bubble is present in the eye, air travel and altitude are strictly contraindicated. The decrease in cabin pressure or at high altitude would cause the bubble to expand, with a major risk of sudden increase in intraocular pressure. A medical certificate can be provided to justify postponing a flight if necessary.
Is the result long-lasting?
After closure, the anatomical result is generally stable over time. OCT allows verification of macular hole healing and the progression of retinal layers. Functional recovery (reading, detail precision) often continues to improve over several months, even after closure is confirmed. Regular follow-up remains recommended, especially if the other eye is affected or in cases of high myopia.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. performs a comprehensive evaluation (fundus examination and macular OCT) and discusses the indication for vitrectomy when necessary, with a detailed explanation of the postoperative course and follow-up.
Book an AppointmentFurther reading
- Macular OCT: the key examination for analyzing the macula.
- Epiretinal membrane: a common cause of traction.
- Vitrectomy: procedure and postoperative course of vitreoretinal surgery.