
Lattice degeneration, also known as palisade retinal degeneration, refers to thin, weakened areas of the peripheral retina, often discovered during a routine fundus examination. It is generally asymptomatic, but can increase the risk of retinal tears and subsequent retinal detachment in certain specific situations. Julien Gozlan, M.D., ophthalmologist in Paris 16, explains what lattice degeneration is, when it should simply be monitored, and in which cases prophylactic laser retinopexy is truly indicated.
What exactly is lattice degeneration?
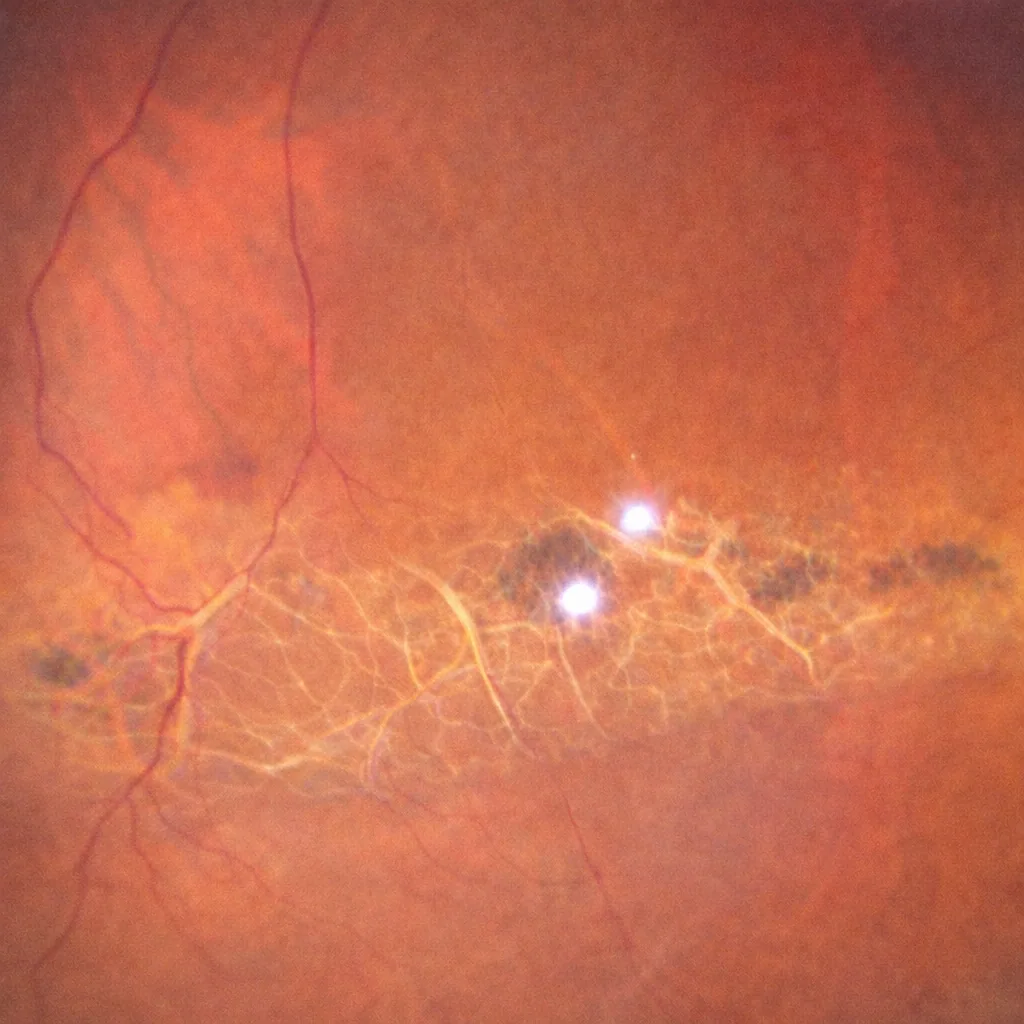
The retina is a thin membrane lining the back of the eye, responsible for receiving light and transmitting visual signals to the brain. In the periphery, there may be areas of degeneration where the retina becomes thinner, sometimes riddled with small holes, with a band-like or lattice appearance. This is referred to as lattice degeneration.
Anatomically, lattice degeneration often corresponds to:
- thinning of the peripheral retina;
- whitish or pigmented patches arranged in parallel bands;
- small atrophic holes or tears within the weakened area;
- vitreous traction sometimes visible at their edges.
These lesions do not necessarily mean that the retina will detach, but they define a zone of weakness where a subsequent event (vitreous traction, trauma, high myopia) can more easily trigger a tear.
Who develops lattice degeneration?
Lattice degeneration is relatively common and can be found in individuals without any particular symptoms. It is more frequently observed in the following situations:
- High or moderate myopia: elongation of the eyeball stretches the peripheral retina and promotes degeneration.
- Adults over 40–50 years old: the vitreous changes and exerts more pronounced traction on certain areas of the retina.
- Personal or family history of retinal detachment: lattice degeneration is more frequently found in these contexts.
- Ocular or cranial trauma: an impact can weaken already predisposed areas.
In most cases, the patient has no symptoms and the lesion is discovered incidentally during a fundus examination performed for myopia, a glasses check-up, or another reason.
Lattice degeneration: symptoms and warning signs
In themselves, lattice degenerations are most often silent. However, they can be the site of a retinal tear when vitreous traction is exerted on this fragile area. Certain symptoms should then raise concern:
- recent onset of unusual floaters (numerous floating bodies, "shower of soot");
- perception of light flashes (photopsia) in the dark or with eyes closed;
- sensation of a shadow, veil, or "curtain" in part of the visual field;
- sudden decrease in vision, especially if the veil appears to be progressing.
These signs do not always indicate a detachment, but they warrant a prompt ophthalmological consultation, ideally within 24 to 48 hours, to check the condition of the retina and look for a tear on or near a lattice lesion.
Diagnosis: fundus examination, wide-field imaging, and OCT
Diagnosis is based on a fundus examination after pupil dilation. The ophthalmologist carefully examines the retinal periphery, sometimes using:
- a three-mirror lens or equivalent;
- scleral indentation to better visualize the most peripheral areas;
- wide-field imaging to document the appearance of the lattice degeneration.
In some cases, a macular or peripheral OCT may complement the examination to analyze vitreous traction, verify the integrity of the macula, and look for associated edema. The objective is to determine:
- the location of the lattice lesions (superior, inferior, temporal, multiple);
- their extent and whether holes or tears are present within the area;
- the presence of signs of early detachment (retinal elevation, subretinal fluid).
Lattice degeneration and the risk of retinal detachment
Not all lattice degenerations lead to retinal detachment. The risk of progression depends on several factors:
- presence of holes or tears within the lattice lesion;
- high myopia or a very elongated globe;
- history of detachment in the fellow eye;
- presence of significant vitreous traction or a recent posterior vitreous detachment;
- recent ocular or cranial trauma.
In limited forms, without an associated hole and in a patient without major risk factors, the prognosis is generally favorable and simple regular monitoring is sufficient. Conversely, when certain criteria are met, prophylactic treatment is much more readily considered.
Should lattice degeneration always be treated?
The answer is no: not all lattice degenerations are systematically treated. The decision is based on a precise assessment of the risk of detachment. In practice, the main situations where laser retinopexy may be indicated are:
- lattice degeneration in a fellow eye when the other eye has already experienced a retinal detachment;
- lattice with holes: presence of one or more holes within the lattice degeneration;
- lattice degeneration in a functionally single eye (monocular patient or poor vision in the other eye).
Outside of these cases, a small lattice lesion without holes, in a mildly myopic patient with no significant history, will most often be simply monitored, with education on warning signs. The onset of recent symptoms (floaters, flashes, veil) may, however, lead to reconsideration of the indication for laser retinopexy.
What does prophylactic laser retinopexy involve?
When one of the following situations is present – lattice degeneration in the fellow eye with a history of contralateral retinal detachment, lattice with holes, or lattice degeneration in a single eye – the ophthalmologist may recommend retinal photocoagulation retinopexy. The principle is to create, around the lattice area and any associated holes, a ring of laser spots to form an adhesive scar between the retina and the eye wall.
The procedure is generally performed in the office:
- instillation of dilating and anesthetic eye drops;
- possible placement of a special contact lens on the eye, with transparent gel;
- application of laser spots around the targeted area.
Light sensitivity, stinging, or a feeling of eye fatigue are possible during and after the session, but most patients describe the procedure as impressive but tolerable. The goal is to reduce the risk of a retinal detachment forming from this fragile area.
Prognosis and long-term follow-up
When properly assessed and, if necessary, protected by laser retinopexy, lattice degeneration generally has a good prognosis. However, there always remains a residual risk of new lesions or tears elsewhere on the retina, particularly in patients with high myopia or a significant family history.
Follow-up often includes:
- a close follow-up visit after treatment, if laser was performed;
- periodic fundus examinations based on the risk profile;
- education on warning signs (sudden floaters, flashes, veil) to seek immediate consultation in the event of new symptoms.
The objective is to detect as early as possible any progression toward a tear or early detachment, in order to treat under optimal conditions.
FAQ: Lattice degeneration
Is lattice degeneration always serious?
No. Lattice degeneration is often an incidental finding, with no immediate consequences for vision. However, it does indicate an area of peripheral weakness, more susceptible to tears in the event of vitreous traction, high myopia, or trauma. This is why it must be monitored, and sometimes protected by laser retinopexy when certain well-defined criteria are present (fellow eye after contralateral detachment, lattice with holes, single eye).
What is the risk of retinal detachment when you have lattice degeneration?
The risk varies greatly from person to person. In a mildly myopic patient without holes or prior history, it can remain low. However, it is higher in cases of lattice degeneration in the fellow eye with contralateral retinal detachment, lattice with holes, or a functionally single eye. In these contexts, prophylactic laser retinopexy is frequently considered. Your ophthalmologist assesses this risk after a detailed fundus examination and imaging.
Should I avoid sports if I have lattice degeneration?
Most gentle or moderate physical activities (brisk walking, leisurely cycling, swimming, gymnastics) remain possible. However, contact sports (boxing, martial arts, rugby) or activities with risk of head impacts should be discussed on a case-by-case basis, especially in highly myopic patients or those with a history of detachment. The goal is to limit trauma that could reactivate traction on the fragile retina.
Can you fly with lattice degeneration?
Yes. The presence of lattice degeneration does not prevent air travel. The main restriction concerns patients who have undergone a vitrectomy with intraocular gas, for whom flying is temporarily contraindicated. If you do not have gas in your eye and no recent surgery has been performed, flying is generally permitted. If in doubt, it is preferable to seek confirmation during a consultation.
Should I automatically have laser treatment if lattice degeneration is found?
No, prophylactic retinopexy is not systematic. It is generally reserved for three main scenarios: lattice degeneration in the fellow eye with a history of contralateral retinal detachment, lattice with holes, and lattice degeneration in a single eye. In mild, stable forms, simple monitoring with education on warning signs is often sufficient. The decision is always made after explanation and discussion with the patient.
If laser treatment has been performed, am I permanently protected?
Laser retinopexy locally reinforces the treated area and significantly reduces the risk of a detachment originating from that lattice lesion. However, it does not prevent the possible appearance of other lesions or tears at a distance, in other sectors of the retina. This is why regular follow-up and vigilance for any new symptoms (sudden floaters, flashes, veil) remain essential even after a well-performed laser treatment.
Can lattice degeneration disappear over time?
Lattice degeneration does not regress spontaneously, but its appearance may stabilize after a certain age, particularly when the posterior vitreous detachment is complete and traction diminishes. The goal is therefore not to make it disappear, but to monitor its progression, treat if necessary, and ensure follow-up appropriate to your risk profile (myopia, family history, ocular surgery, etc.).
When to consult Julien Gozlan, M.D.?
You may seek an opinion if lattice degeneration has been identified during a fundus examination, if you are highly myopic, or if you are experiencing recent symptoms such as unusual floaters, light flashes, or the appearance of a veil in your visual field. A consultation is also recommended in cases of personal or family history of retinal detachment.
Julien Gozlan, M.D., ophthalmologist in Paris 16, performs a thorough fundus examination, supplemented if needed by wide-field imaging and OCT, then discusses with you the most appropriate strategy: simple monitoring, education on warning signs, or prophylactic laser retinopexy when justified.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. sees you at the Paris – Auteuil Ophthalmology Practice to evaluate your lattice degeneration, assess the risk of retinal detachment, and establish, if needed, a personalized treatment and follow-up plan.
Book an AppointmentFurther reading
- Retinal detachment: warning signs and surgical management.
- Retinal tear: symptoms, diagnosis, and treatment.
- Laser and the retina: indications for prophylactic retinopexy and other photocoagulation treatments.
- Macular OCT: the reference imaging modality for retinal analysis and vitreous traction assessment.