
Central retinal vein occlusion (CRVO) is an ophthalmological emergency that causes vision loss, which may be more or less sudden, related to impaired blood drainage from the retina. Julien Gozlan, M.D. explains the causes, symptoms, useful examinations, and current treatments for this eye condition.
What is central retinal vein occlusion?
Central retinal vein occlusion (CRVO) occurs when the main vein draining the retina becomes blocked. Blood pools, upstream venous pressure increases, and blood fluid can leak from the blood vessels within the central retina, leading to macular edema responsible for vision loss. There are ischemic forms (poorly perfused, more severe) and non-ischemic forms.
Symptoms of CRVO: when should you seek medical attention?
The most common sign is a decrease in central vision in one eye, with rapid onset, sometimes accompanied by distortion of lines or floaters (myodesopsia) if blood diffuses into the vitreous. In the presence of these signs, a prompt consultation is essential: a central retinal vein occlusion requires an immediate workup.
Risk factors and causes
- High blood pressure,
- Glaucoma and ocular hypertension,
- Diabetes, hypercholesterolemia, smoking,
- Blood hyperviscosity, coagulation disorders,
- Age > 55 years, but central retinal vein occlusion can sometimes affect younger individuals.
In diabetic patients, diabetic macular edema can also worsen visual impairment and requires close monitoring.
Control of general risk factors is essential: blood pressure, metabolic workup, and, if needed, hematological evaluation.
How is the diagnosis confirmed?
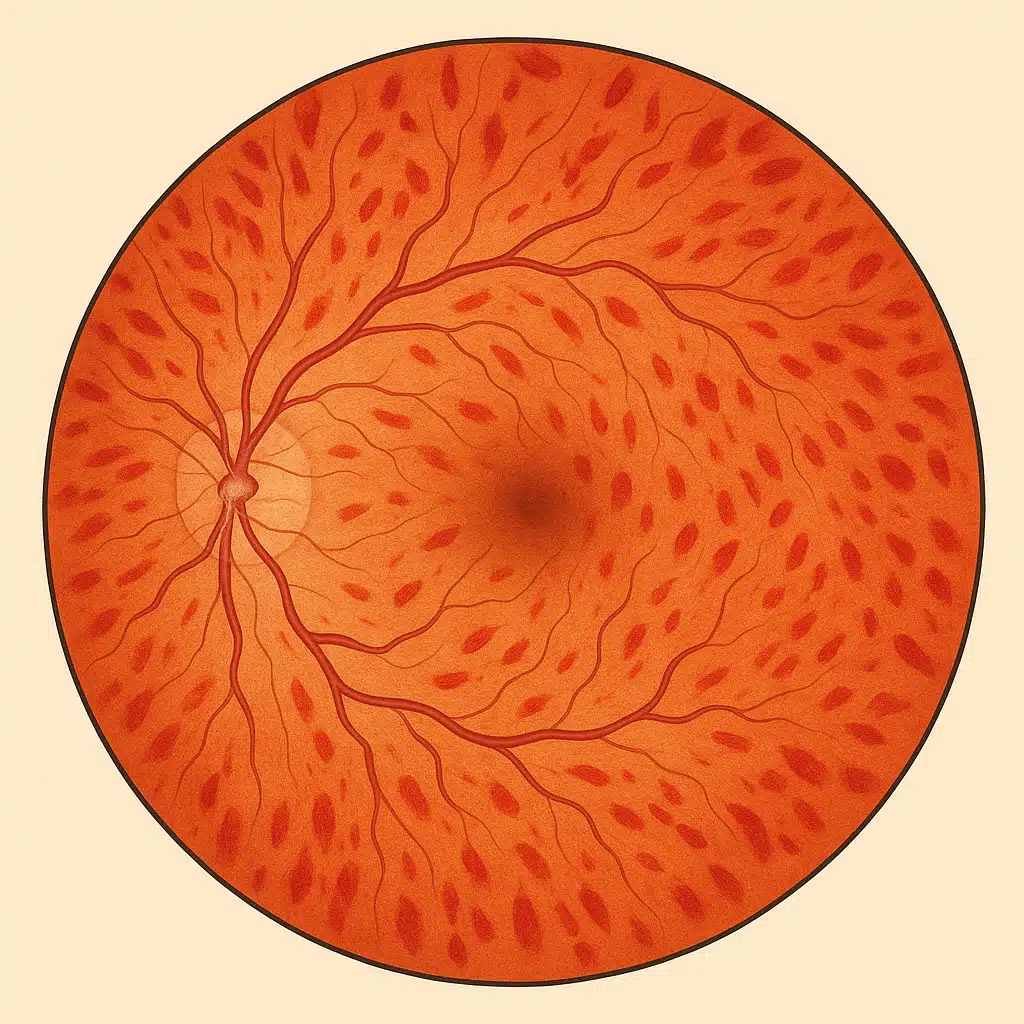
Fundus examination reveals retinal hemorrhages, tortuous and dilated retinal veins, and sometimes a thickened macula. Two imaging examinations guide management:
- Macular OCT: measures the thickness and structure of the macula, detects and evaluates macular edema, and monitors treatment effectiveness.
- Fluorescein retinal angiography: assesses perfusion, identifies areas of ischemia, and detects abnormal blood vessels (neovascularization).
These examinations are repeated during the follow-up of a central retinal vein occlusion (CRVO) to monitor the disease and adjust treatment.
Treatments for central retinal vein occlusion
Intravitreal injections (anti-VEGF / corticosteroids)
The standard treatment for central retinal vein occlusion (CRVO) with macular edema relies on intravitreal injections of anti-VEGF agents or corticosteroids depending on the patient's profile. With anti-VEGF agents, the protocol often begins with 3 monthly injections, then the frequency is adjusted according to treatment response.
Targeted retinal laser
In cases of extensive retinal non-perfusion or neovascularization on angiography, laser photocoagulation may be proposed to reduce the risk of intravitreal hemorrhage, tractional retinal detachment, and neovascular glaucoma.
General management
At the same time, contributing factors are addressed: high blood pressure, glaucoma or ocular hypertension, blood sugar, cholesterol, and smoking cessation. This comprehensive approach reduces the risk of recurrence and protects the fellow eye.
Visual outcome and prognosis
The prognosis depends on initial retinal perfusion and the speed of treatment. In many cases, central retinal vein occlusion (CRVO) can be stabilized with vision improvement when the macular edema resolves. Regular follow-up is essential, as some forms require injections over several months, sometimes years.
Follow-up after CRVO: what to expect?
Clinical examinations and OCT scans are scheduled to adjust the frequency of injections and detect complications (neovascularization, tractional retinal detachment, neovascular glaucoma). The schedule is personalized: more frequent at the beginning, then spaced out if all goes well.
FAQ: frequently asked questions about central retinal vein occlusion (CRVO)
Is CRVO always an absolute emergency?
Yes, a central retinal vein occlusion is considered an ophthalmological emergency, even if vision remains partially usable. In practice, it is not a "minute-by-minute" emergency, but it is important to be seen within the days following the onset of symptoms in order to confirm the diagnosis, assess retinal perfusion, and promptly begin management (intravitreal injections, close monitoring). The earlier the macular edema is treated, the better the chances of a favorable visual prognosis.
Can "normal" vision be recovered after CRVO?
Recovery depends primarily on the initial severity (ischemic or non-ischemic form), the condition of the macula, and the speed of management. Some patients regain very satisfactory vision for daily life, while others retain a visual deficit (decreased acuity, distortion, reduced contrast). The goal of treatment is to stabilize and improve vision as much as possible, but it is not always possible to return to the situation "before" the episode. This is discussed on a case-by-case basis depending on imaging findings and treatment response.
Is the fellow eye at risk of being affected as well?
The risk of CRVO in the fellow eye exists, especially if general risk factors are not corrected (high blood pressure, diabetes, hypercholesterolemia, coagulation disorders, smoking, glaucoma). However, it remains low if these factors are well controlled. This is why an occlusion in one eye should always be accompanied by preventive measures for the fellow eye: regular monitoring of blood pressure and intraocular pressure, vascular workup, healthy lifestyle, and scheduled ophthalmological follow-up even in the absence of symptoms.
Is CRVO related to a heart condition or stroke risk?
A central retinal vein occlusion most often reflects fragility of the retinal venous circulation, in the context of an underlying cardiovascular condition (hypertension, cardiac arrhythmia, diabetes, dyslipidemia, smoking, coagulation disorders, etc.). It is not a stroke in the strict sense, but it can be a marker of an at-risk vascular profile. This is why the ophthalmologist often refers the patient to the primary care physician or cardiologist for a comprehensive workup and potential adjustment of preventive treatments (blood pressure, cholesterol, possible antiplatelet or anticoagulant therapy depending on the case).
Will I be able to continue working and driving after CRVO?
It all depends on the level of vision achieved after treatment and the type of occupation. If the fellow eye has good vision, returning to work is often possible, sometimes with some adjustments (lighting, visual breaks, optical aids). For driving, the legal binocular visual acuity thresholds must be met, and contrast perception and visual field must remain sufficient. In some cases, a restriction on night driving or long-distance driving may be recommended. These decisions are made during consultations, based on visual examinations and your day-to-day safety.
Are intravitreal injections painful and always necessary?
Intravitreal injections are performed under local anesthesia with eye drops, under strict aseptic conditions. Most patients describe a brief sensation of discomfort lasting a few seconds, but no real pain. They are indicated when there is significant macular edema and the goal is to limit vision loss. In certain forms with very few symptoms or minimal edema, monitoring alone may be considered, but regular injections remain the cornerstone of treatment for many cases of CRVO. The strategy (frequency, drug, duration) is adjusted according to the OCT findings and tolerability.
Can CRVO recur after a first episode?
A new occlusion in the same eye is uncommon but not impossible, particularly if vascular risk factors are not corrected. However, chronic macular edema may persist or recur, requiring injections over time, sometimes with phases of improvement and relapse. Follow-up is precisely intended to adjust treatment in order to anticipate these reactivations and intervene before significant vision loss occurs. In the long term, controlling general risk factors is just as important as the ocular treatments themselves.
What long-term follow-up is needed after central retinal vein occlusion?
Follow-up includes regular ophthalmological consultations with visual acuity measurement, fundus examination, and macular OCT to monitor edema, perfusion, and the possible development of neovascularization. The frequency is close together during the first months (every 1 to 2 months), then may be spaced out if the condition stabilizes. At the same time, follow-up with the primary care physician, cardiologist, or endocrinologist is essential to control blood pressure, blood sugar, cholesterol, and weight. This dual follow-up (eye and general risk factors) aims to protect long-term vision and reduce the risk of vascular events elsewhere in the body.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. performs the workup for central retinal vein occlusion: clinical examination, macular OCT, angiography if necessary, and intravitreal injections according to a personalized protocol.
Book an AppointmentFor additional general information, you may also consult the page dedicated to retinal vein occlusions on the Retina France website.
Further reading
- Macular OCT: the reference imaging technique for monitoring macular edema.
- Intravitreal injections: procedure, efficacy, and safety.
- Vitrectomy: specific indications in case of complications.