
Central serous chorioretinopathy (CSC) is a retinal disease that primarily affects young or middle-aged adults, often those under stress and sometimes taking corticosteroids. It manifests as a small serous detachment of the macula, causing blurred and distorted vision. Julien Gozlan, M.D., ophthalmic surgeon in Paris 16, explains the symptoms, the role of OCT, and the treatments for CSC.
What is CSC?
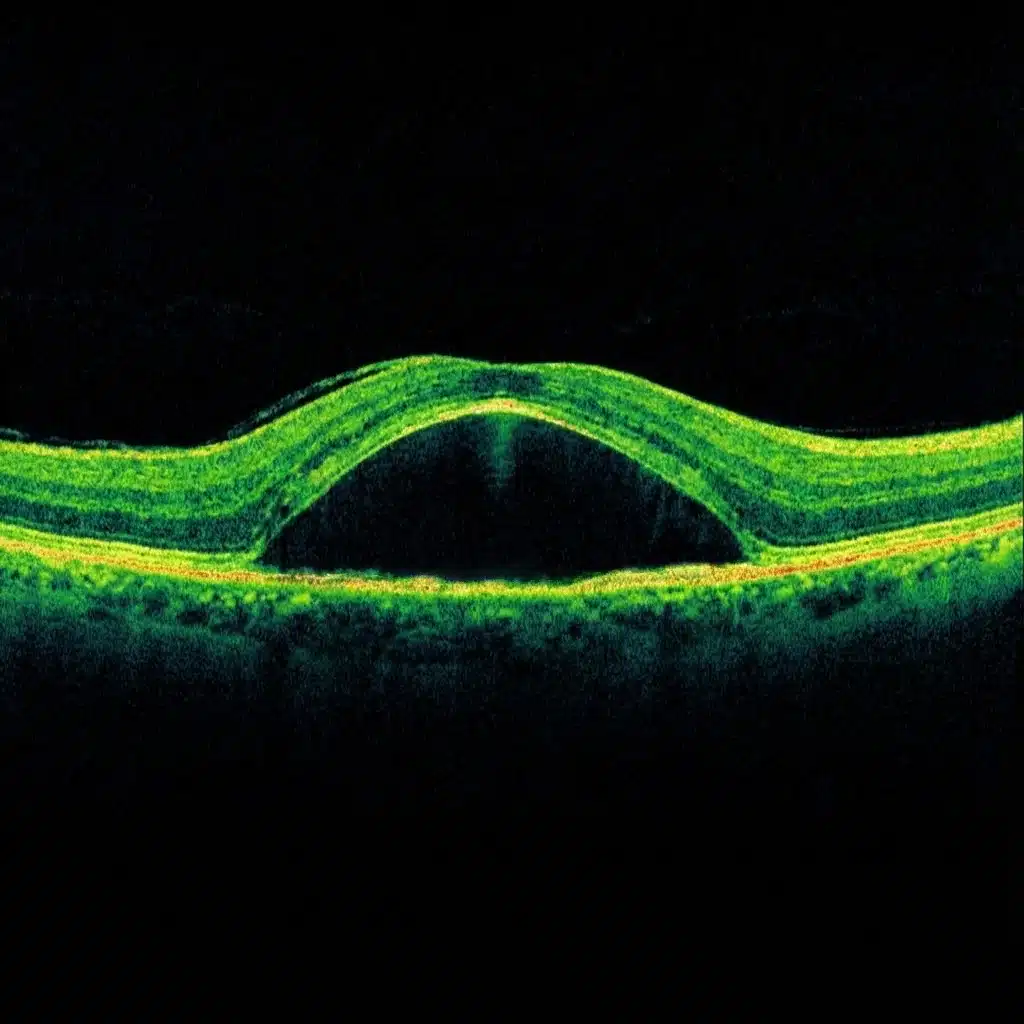
Central serous chorioretinopathy is a macular condition in which fluid accumulates beneath the neurosensory retina, creating a small serous detachment blister at the center of the fundus. The macula is slightly elevated, which disrupts image focusing.
CSC more frequently affects men between the ages of 30 and 60 but can also occur in women. It is most often unilateral at onset, but the fellow eye should be monitored.
Symptoms of central serous chorioretinopathy
The typical symptoms of CSC are:
- central blurred vision in one eye, sometimes described as "like looking through water";
- distortion of lines (metamorphopsia): straight lines appear wavy;
- a sensation that a letter is missing in the center of words;
- micropsia: objects appear smaller or farther away with the affected eye;
- slightly different color perception between the two eyes.
These signs should prompt a consultation, especially if they occur recently in a patient under stress or using corticosteroids (tablets, sprays, ointments, injections, etc.).
How is the diagnosis made?
Fundus examination may reveal an unusual reflex or a raised area at the macula. The key examination is macular OCT, which demonstrates the serous detachment of the retina and allows its extent to be measured.
In some cases, the workup is supplemented by indocyanine green angiography, to analyze the choroidal circulation and identify areas of hyperpermeability characteristic of the "pachychoroid spectrum." Fluorescein angiography may also be performed depending on the clinical context.
Causes and risk factors of CSC
Central serous chorioretinopathy is related to dysfunction of the choroid (the vascular layer beneath the retina) and the retinal pigment epithelium, which allow fluid to seep beneath the macula. Several risk factors are recognized:
- chronic stress, anxious personality, or overwork;
- corticosteroid use (oral, inhaled, topical, injections, etc.);
- sleep disturbances and night-shift work;
- high blood pressure or other cardiovascular risk factors;
- pachychoroid phenotype (thickened choroid) observed on imaging.
In some cases, no obvious cause is identified. The clinical history and workup aim to identify modifiable factors, particularly corticosteroids, when they are not essential.
Natural course of CSC
In many cases, acute CSC resolves spontaneously within a few weeks to a few months: the fluid reabsorbs, the macula reattaches, and vision gradually improves. However, a slight difference in perception between the two eyes may persist.
Some forms become chronic or recurrent, with fluid that persists or returns multiple times. Over the long term, damage to the retinal pigment epithelium and retina can then lead to more lasting vision loss, underscoring the importance of regular follow-up.
Treatments for central serous chorioretinopathy
Simple monitoring and general measures
When visual acuity remains adequate and the episode is recent, simple monitoring is often recommended, especially during a first episode. The goal is to observe spontaneous fluid resorption on OCT.
At the same time, the physician may recommend:
- reducing or discontinuing corticosteroids if possible, in agreement with the prescribing physician;
- addressing stress, sleep, and lifestyle habits;
- monitoring near vision regularly, one eye at a time, using an Amsler grid.
Targeted treatments (laser, photodynamic therapy)
In chronic forms, those that are highly bothersome, or those threatening central vision, targeted treatments may be offered, based on the angiographic and OCT findings:
- gentle focal laser applied to a well-identified leak, away from the macular center;
- photodynamic therapy (PDT) at reduced dose, which targets areas of choroidal hyperpermeability.
In certain situations where choroidal neovascularization is present, intravitreal injections of anti-VEGF agents may be considered.
Follow-up and prognosis
In the majority of cases, acute central serous chorioretinopathy has a good visual prognosis, with satisfactory functional recovery. The prognosis is more guarded in chronic forms, cases with multiple recurrences, or longstanding lesions.
Follow-up consists of regular check-ups including visual acuity measurement and macular OCT, to verify the disappearance or reappearance of fluid. Patients are encouraged to monitor their own vision (reading, Amsler grid) and to report any new distortion or vision loss in the affected eye.
Practical advice for patients with CSC
If you have CSC, a few simple measures can help protect the macula and reduce the risk of recurrence:
- discontinue corticosteroid treatments if possible, in consultation with your treating physician;
- maintain a regular sleep schedule and healthy lifestyle habits;
- reduce chronic stress (physical activity, relaxation, professional support if needed);
- test your near vision regularly, one eye at a time;
- seek prompt consultation if you notice new distortion or decreased vision.
FAQ: central serous chorioretinopathy (CSC)
Is CSC an ophthalmic emergency?
In most cases, CSC is not a sight-threatening emergency, as it involves a serous detachment of the macula that typically evolves over several weeks. However, recent vision loss, distortion (metamorphopsia), or worsening symptoms warrant a prompt consultation to confirm the diagnosis with OCT and to rule out other causes (particularly associated neovascularization).
What are the typical symptoms of CSC?
The most common symptoms are central blurred vision in one eye, wavy lines (metamorphopsia), a sensation that a word is "missing" in the center, micropsia (objects appear smaller), and sometimes slightly different color perception between the two eyes. Many patients describe their vision as "like looking through water."
Can CSC resolve on its own?
Yes, in many cases. Acute CSC resolves spontaneously within a few weeks to a few months: the fluid reabsorbs, the macula reattaches, and vision improves. However, a slight difference in image quality between the two eyes may persist. If the fluid persists or recurs, this is referred to as a chronic or recurrent form, which requires more targeted management.
What role do corticosteroids play in CSC?
Corticosteroids are a well-established risk factor for CSC, regardless of their form: tablets, inhalers, nasal sprays, creams/ointments, or injections. They can trigger an episode or perpetuate a chronic form. If CSC is diagnosed, any corticosteroid use should be reported, and a reduction or discontinuation should be discussed with the prescribing physician whenever possible and medically appropriate.
Why is OCT the key examination in CSC?
Macular OCT allows direct visualization of subretinal fluid, measurement of the extent of serous detachment, and monitoring of its progression over time. It also helps identify signs suggestive of a more chronic form (retinal pigment epithelium changes, more diffuse abnormalities) and to detect complications such as choroidal neovascularization when the presentation is atypical or persistent.
What are the purposes of fluorescein angiography and indocyanine green angiography?
Angiography can be useful to locate a leak, analyze the choroid, and confirm the context of a pachychoroid phenotype. Indocyanine green angiography often reveals areas of choroidal hyperpermeability, which helps guide treatment, particularly when photodynamic therapy (PDT) is being considered. Depending on the case, fluorescein angiography may also be performed to clarify the mechanism and rule out other diagnoses.
When is treatment recommended rather than simple monitoring?
Monitoring is often recommended for a first recent episode with adequate visual acuity, as spontaneous resolution is common. Treatment is considered if the fluid persists, if the form becomes chronic, if the impairment is significant, if the episode recurs, or if imaging suggests a lasting threat to the macula (retinal pigment epithelium changes, more diffuse involvement).
What are the possible treatments for CSC?
The options depend on the clinical profile (acute, chronic) and imaging findings. Monitoring and general measures (stress management, sleep optimization, discontinuation of corticosteroids if possible) may be recommended. In more bothersome or persistent forms, gentle focal laser may be considered if the leak is well identified and located away from the macular center. Photodynamic therapy (PDT) at reduced dose is a common option for chronic forms associated with choroidal hyperpermeability. If neovascularization is present, intravitreal injections of anti-VEGF agents may be indicated.
Is there a risk of recurrence?
Yes, CSC can recur, sometimes in the same eye, sometimes in the fellow eye. The risk is higher if contributing factors persist (significant stress, sleep disturbances, corticosteroids). This is why follow-up with OCT, self-monitoring (reading, Amsler grid), and management of risk factors are important, even after improvement.
When should you seek prompt follow-up in case of CSC?
You should seek prompt consultation if you experience new vision loss, worsening distortion, the appearance of a more prominent central dark spot, or if symptoms occur while taking corticosteroids. Rapid deterioration may indicate a recurrence, persistent fluid, or more rarely a complication (neovascularization), warranting a timely check-up.
When to consult Julien Gozlan, M.D.
You may seek a specialist opinion if you notice central blurred vision, wavy lines, a difference in vision between the two eyes, or if another physician has mentioned central serous chorioretinopathy. Patients under stress, taking corticosteroids, or already being followed for a macular condition should be particularly vigilant.
Julien Gozlan, M.D., ophthalmologist in Paris 16, performs a comprehensive evaluation (clinical examination, OCT, retinal imaging) and proposes a personalized strategy: simple monitoring, general measures, or targeted treatment if necessary.
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Julien Gozlan, M.D. welcomes you at Paris – Auteuil Ophthalmology Practice for the diagnosis, follow-up, and treatment of central serous chorioretinopathy (CSC) and other macular diseases.
Book an AppointmentFurther reading
- Macular OCT: the reference examination for analyzing the macula.
- Indocyanine green angiography: choroidal imaging in pachychoroid spectrum diseases.
- Intravitreal injections: imaging-guided retinal treatments.