
Posterior vitreous detachment is a very common condition after the age of 50. The transparent gel that fills the eye, the vitreous, gradually detaches from the retina. In the majority of cases, the phenomenon is benign, but it can sometimes be accompanied by a retinal tear. Dr Julien Gozlan, ophthalmic surgeon in Paris 16, explains the symptoms, risks, and necessary monitoring.
What are the vitreous and posterior vitreous detachment?
Inside the eye, behind the lens, there is a transparent gel called the vitreous. This gel is surrounded by a thin membrane that adheres to the retina, especially at the periphery and at the macula. With age, the vitreous liquefies and the membrane covering it gradually detaches from the retinal surface: this is posterior vitreous detachment.
This is most often a phenomenon related to normal aging of the eye. It can occur earlier in myopic individuals, after cataract surgery, or following ocular trauma.
Symptoms: when should you be concerned?
The typical signs of posterior vitreous detachment are:
- the sudden appearance of "floaters" in greater numbers;
- flashes of light on the side of the visual field, especially in the dark;
- sometimes, the perception of a ring or moving shadow that shifts with eye movement.
These symptoms can be alarming but do not necessarily indicate a complication. However, the appearance of a dark curtain or a "veil" progressing across the visual field suggests a retinal detachment and requires an emergency consultation.
Why can posterior vitreous detachment be risky?
As it detaches, the vitreous briefly pulls on certain attachment points to the retina. In most cases, this traction leaves no lasting damage. In others, it can cause a retinal tear, particularly if the retina is thin, myopic, or already weakened.
A tear is a small opening in the retina through which fluid can pass and create a retinal detachment. This is why any recent posterior vitreous detachment, with clear symptoms, warrants a comprehensive fundus examination.
How is the diagnosis made?
The ophthalmologist begins by measuring visual acuity and examines the fundus after pupil dilation. They look for signs of posterior vitreous detachment (Weiss ring, vitreous condensation) and carefully inspect the retinal periphery with a slit lamp, sometimes using a special lens.
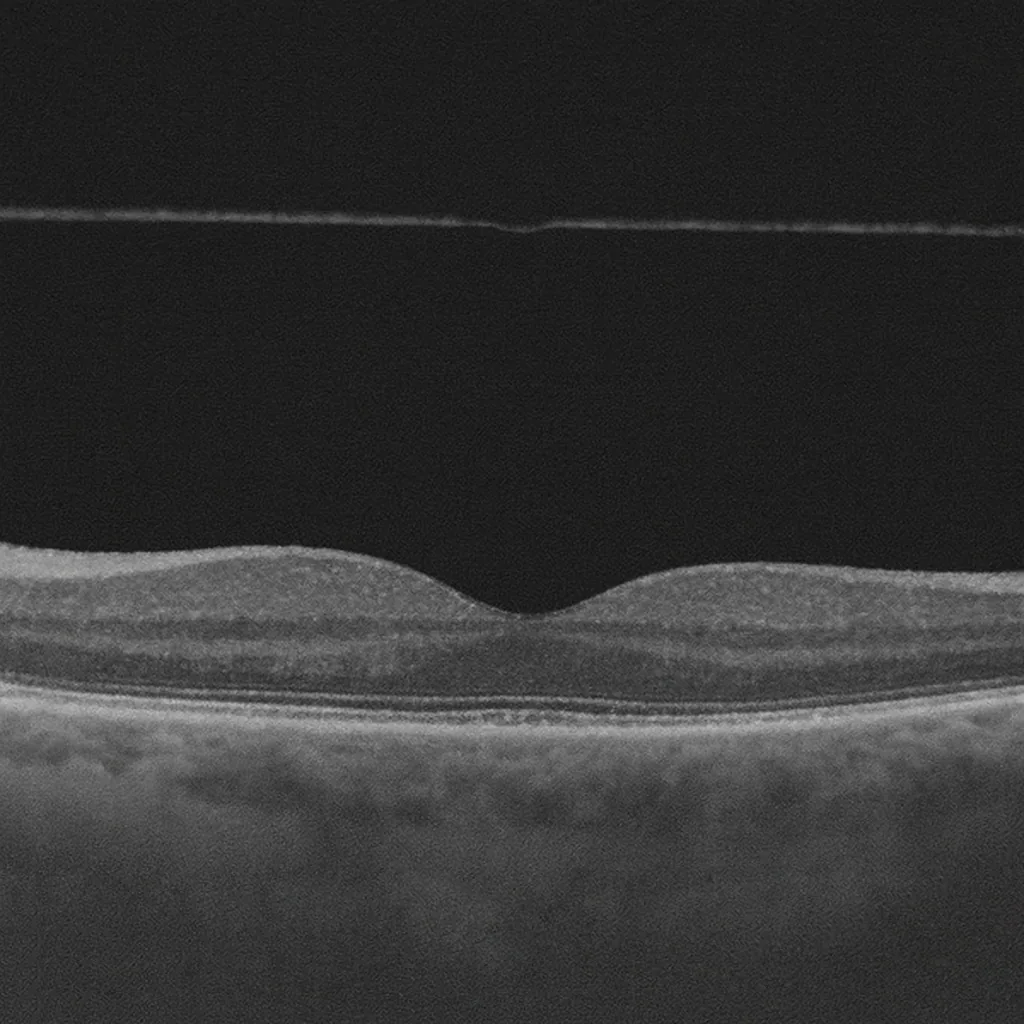
If the ocular media lack transparency (dense cataract, intravitreal hemorrhage), an ocular ultrasound may be performed to verify that no retinal detachment is present. Macular OCT is useful if traction at the macula or a complication such as a macular hole is suspected.
Typical progression and monitoring
In most cases, posterior vitreous detachment stabilizes within a few weeks. Floaters may remain visible but become less bothersome as the brain gradually learns to ignore them. Flashes of light diminish and then disappear.
When the initial examination reveals neither a tear nor a retinal detachment, monitoring is still recommended, especially during the first few months. The patient should return for an emergency consultation if a new episode of a "shower" of floaters, repeated flashes, or a curtain in the visual field occurs.
What are the treatments?
Posterior vitreous detachment itself generally does not require treatment: it is a natural stage in the life of the eye. What is treated are the potential complications:
- a retinal tear is treated with emergency laser therapy to prevent a retinal detachment;
- a confirmed retinal detachment requires surgery;
- rare cases of significant macular traction may warrant a vitrectomy.
Isolated floaters are generally not treated surgically. Simple measures (adequate hydration, visual breaks, appropriate lighting) can help patients cope with them on a daily basis.
Practical advice for patients
If a posterior vitreous detachment has been diagnosed, it is recommended to:
- watch for the appearance of a dark curtain or a sudden decrease in vision;
- seek prompt medical attention if new flashes or a shower of floaters occur;
- continue regular ophthalmological follow-up, especially in cases of high myopia or a history of retinal detachment.
These guidelines help detect complications early and intervene at the right time.
FAQ: frequently asked questions about posterior vitreous detachment
Is posterior vitreous detachment an emergency?
Posterior vitreous detachment itself is generally not a sight-threatening emergency. However, the sudden onset of symptoms (numerous floaters, flashes of light, dark curtain) should prompt you to seek medical attention promptly. The goal is to verify that there is no associated retinal tear or retinal detachment, which do require urgent treatment.
What signs should concern me in case of posterior vitreous detachment?
The signs that require a prompt consultation are:
- the sudden, shower-like appearance of floaters;
- the perception of flashes of light in one eye;
- the sensation of a dark veil or curtain obscuring part of the visual field;
- an unusual or rapid decrease in vision.
These symptoms may indicate a retinal tear or the onset of a retinal detachment, and should be examined without delay.
Will posterior vitreous detachment permanently impair my vision?
In the majority of cases, posterior vitreous detachment is a phenomenon related to normal aging of the eye. It mainly causes floaters and sometimes a few flashes at the beginning. After a few weeks or months, the brain adapts and the discomfort decreases significantly. Vision may remain slightly disturbed by certain opacities, but in the absence of a retinal complication, there is no permanent loss of central vision.
Is there a treatment to make floaters disappear?
To date, there is no simple and routine treatment to eliminate all floaters. In the vast majority of cases, the approach relies on the brain's adaptation and the spontaneous decrease in discomfort over time.
Surgical procedures (vitrectomy) may be considered in rare cases of severe and debilitating symptoms, but they are not offered routinely, as they carry their own risks. The main priority remains verifying the integrity of the retina.
Does posterior vitreous detachment increase the risk of retinal detachment?
Yes, during the phase of recent posterior vitreous detachment, there is a risk of traction on the retina that can cause a retinal tear, which in turn can lead to a retinal detachment. This risk is higher in individuals with high myopia, after ocular trauma, or if there is a history of retinal detachment in the other eye. Hence the importance of a comprehensive fundus examination during the initial phase, and sometimes a follow-up examination at a later date.
Can I drive, play sports, or fly with posterior vitreous detachment?
In the absence of retinal complications and if visual acuity remains adequate, driving and most activities can be continued. However, floaters may be more bothersome in bright light or against a light background: it is wise to be more cautious when driving at first.
Posterior vitreous detachment does not prevent you from flying. However, if a tear or a retinal detachment is discovered, driving, sports, and sometimes travel will need to be adjusted depending on the treatment required.
When should you consult Dr Julien Gozlan?
If you suddenly notice a large number of floaters, flashes of light, or a curtain in your visual field, it is important to seek prompt medical attention. Even though posterior vitreous detachment is often benign, only a comprehensive examination can confirm the absence of a tear or retinal detachment.
Dr Julien Gozlan, ophthalmologist in Paris 16, performs a detailed assessment (fundus examination, OCT, ultrasound if needed) and arranges the monitoring or treatment best suited to your situation.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan welcomes you at the Paris – Auteuil Ophthalmology Practice for the diagnosis and follow-up of posterior vitreous detachment and other retinal and vitreous conditions.
Book an AppointmentFurther reading
- Floaters: understanding eye floaters.
- Retinal detachment: warning signs and management.
- Macular OCT: a key examination for analyzing the retina and vitreous.