
Before cataract surgery, corneal topography has become a standard examination. It allows precise analysis of the shape and regularity of the cornea, screening for certain conditions, and optimizing the choice of intraocular lens. Dr Julien Gozlan, ophthalmic surgeon in Paris 16, explains how corneal topography makes cataract surgery safer and more personalized.
What is corneal topography?
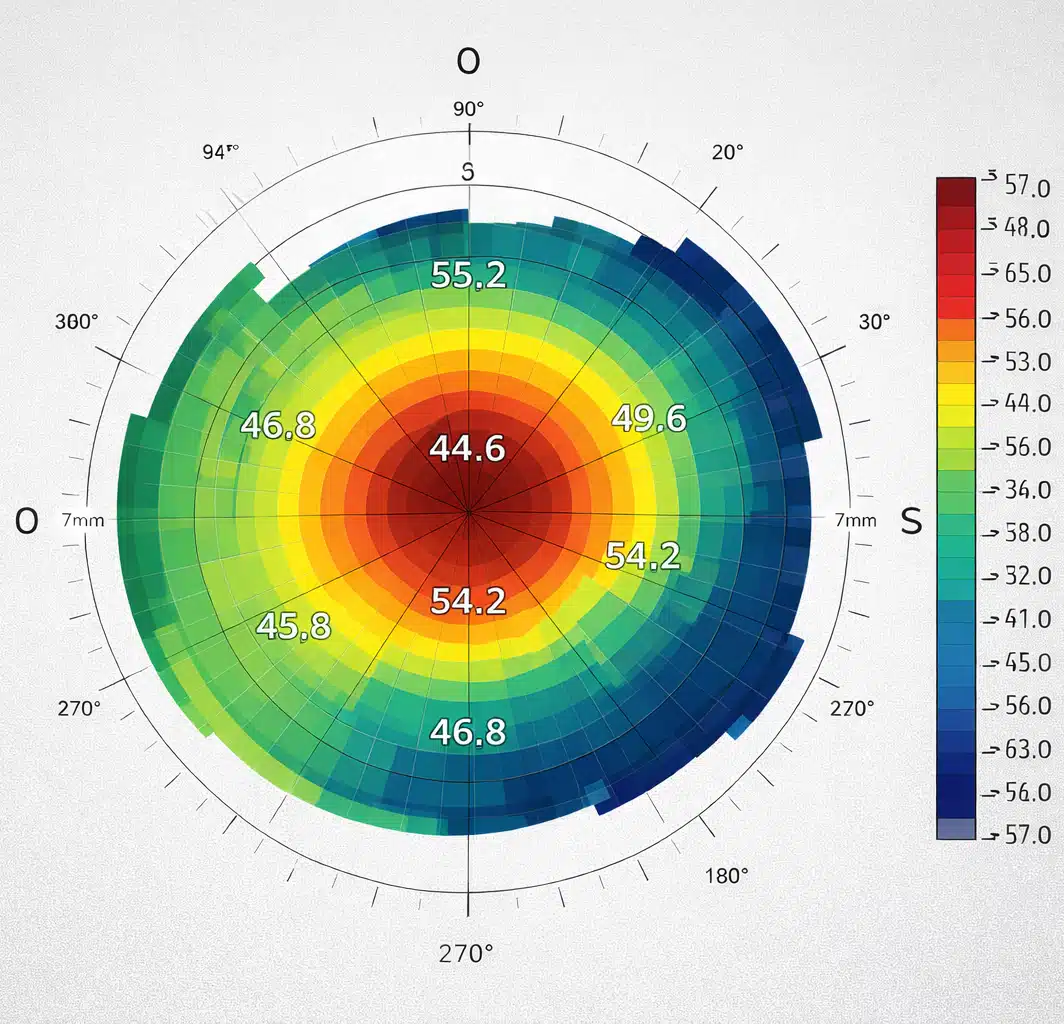
Corneal topography is an imaging examination that maps the surface of the cornea. It measures its curvature point by point and generates color-coded maps showing areas of greater or lesser curvature. It is sometimes referred to as a "relief map" of the cornea.
This examination is completely painless: the patient looks at a fixed point in the device for a few seconds, with no contact with the eye. Corneal topography is particularly useful for patients who are about to undergo cataract surgery, but also in contact lens fitting, refractive surgery, and for monitoring certain corneal conditions.
Why perform corneal topography before cataract surgery?
Before cataract surgery, it is essential to have a thorough understanding of the corneal shape. The main objectives are:
- precisely measuring corneal astigmatism (magnitude and axis);
- screening for keratoconus or other structural abnormalities;
- detecting corneal irregularities (which may limit the outcome);
- ensuring the suitability of a "premium" lens (multifocal, EDOF, toric) by verifying corneal compatibility.
This information allows the surgical plan to be tailored: type of lens, potential astigmatism correction, and the patient's visual expectations (distance vision only, distance/near compromise, maximum reduction of glasses dependence). Accurate corneal topography directly contributes to the quality of the visual outcome after cataract surgery.
How is corneal topography performed?
The examination is carried out at the practice, seated in front of the device, much like a standard eye examination. Pupil dilation is not required. You are simply asked to fixate on a light point and remain still for a few seconds.
The machine projects luminous rings onto the cornea and analyzes the way they are reflected. The data are then processed by software that generates several maps (curvature, elevation, and sometimes thickness depending on the device). Dr Julien Gozlan interprets these maps to verify that the cornea is regular, stable, and well-centered before cataract surgery.
Topography: what elements are actually assessed before cataract surgery?
Beyond the "color-coded appearance," the analysis is based on several very specific points. Before cataract surgery, particular attention is paid to:
- total astigmatism and its axis (stability, regularity);
- whether the astigmatism is regular or irregular;
- the presence of asymmetry or a suspicious area suggestive of early keratoconus;
- map consistency (repeatability) and measurement quality (fixation, tear film);
- with certain devices (such as the Pentacam), elevation maps and ectasia risk indices.
This analysis is essential because cataract can be treated very effectively, but the final visual outcome also depends on the optical quality of the cornea.
Corneal topography: typical findings
In practice, corneal topography provides several complementary maps, some of which are particularly useful before cataract surgery:
- Axial / curvature map: shows the distribution of corneal power, useful for evaluating astigmatism and its axis.
- Tangential map: more sensitive to local irregularities, valuable for detecting early keratoconus.
- Elevation maps (relative to a sphere or ellipsoid): highlight areas of protrusion or depression, typical of certain ectasias.
- Thickness / pachymetry maps: show areas of thinning, important in cases of keratoconus or prior refractive surgery.
- Global regularity indices: help quantify irregular astigmatism and assess compatibility with certain lenses.
These "topographic findings" make it possible to anticipate the optical quality of the cornea after cataract surgery and to adjust the choice of intraocular lens.
What abnormalities can topography reveal?
Corneal topography can detect numerous situations that may influence the outcome of cataract surgery:
- astigmatism greater than that measured by spectacle refraction alone;
- early or more advanced keratoconus;
- an irregular cornea following refractive surgery or trauma;
- significant dry eye disease that can distort measurements;
- fragile areas that may predispose to corneal decompensation in certain patients.
In some cases, these abnormalities lead to adjustments in the lens choice or to favoring a specific visual target (for example, better distance vision, even if glasses are still needed for reading).
Topography, biometry, and OCT: a comprehensive preoperative assessment before cataract surgery
Corneal topography is part of a broader preoperative assessment. Ocular biometry is used to calculate the lens power based on the axial length of the eye and corneal parameters. A macular examination, often by macular OCT, checks for the absence of underlying retinal pathology (macular edema, age-related macular degeneration, etc.).
In certain patients, particularly those at risk of age-related macular degeneration (AMD), this comprehensive assessment helps to better explain the visual prognosis: the cataract can be removed, but the final quality of vision will also depend on the condition of the retina.
Decision criteria before cataract surgery
The information obtained from corneal topography is decisive in defining the cataract strategy:
- Regular corneal astigmatism: possible indication for a toric lens, with precise calculation of the axis and power to be corrected.
- Irregular astigmatism: caution with multifocal/EDOF lenses, priority given to contrast and visual comfort.
- Keratoconus or ectasia: more conservative strategy, adapted visual goals, sometimes maintaining correction with glasses or rigid contact lenses.
- History of LASIK/PRK: verification of topographic stability and use of specific calculation formulas.
- Significant dry eye disease: prior treatment, then repeat topography before finalizing lens choices.
The goal is to use corneal topography not only as a screening tool, but as a true decision-support instrument to personalize cataract surgery.
Impact on lens selection and astigmatism correction
Corneal topography data are critical for selecting the intraocular lens:
- in cases of regular astigmatism, a toric lens can correct some or all of the astigmatism;
- if the cornea is irregular or shows keratoconus, certain multifocal lenses are avoided in favor of better visual quality and contrast;
- in cases of prior refractive surgery (LASIK, PRK), topography helps interpret measurements and select specific calculation formulas.
The goal is to achieve the most predictable outcome possible, reducing the need for glasses while preserving visual comfort after cataract surgery.
Limitations of corneal topography
This examination does not replace a complete clinical examination of the cornea and anterior segment. Certain situations (corneal scars, edema, significant dry eye disease) can affect measurements and may require repeating the examination or performing additional tests.
Despite these limitations, corneal topography provides essential information for tailoring cataract surgery and anticipating possible visual outcomes.
Prognosis: what impact on vision after surgery?
When the cornea is regular and the retina is healthy, the outcome after cataract surgery is generally excellent. However, an irregular cornea, keratoconus, or an unstable ocular surface can limit:
- the accuracy of astigmatism correction;
- visual comfort (fluctuation, halos, reduced contrast);
- the expected benefit of a multifocal/EDOF lens.
This is why corneal topography is one of the most useful examinations for personalizing the procedure and setting realistic expectations regarding visual outcomes after cataract surgery.
FAQ
Is corneal topography mandatory before cataract surgery?
It is not "mandatory" in an administrative sense, but it has become a standard examination for ensuring the safety of cataract surgery. It allows precise measurement of corneal astigmatism, screening for an irregular cornea (early keratoconus, sequelae of refractive surgery, scarring) and avoiding refractive surprises. In practice, it is particularly useful whenever a "customized" result is desired and/or a toric, EDOF, or multifocal implant is being considered.
What is the difference between biometry and corneal topography?
Ocular biometry is primarily used to calculate the power of the implant (axial length, keratometry, anterior chamber depth, etc.) in order to target the desired correction. Corneal topography provides a more detailed analysis of the shape and regularity of the cornea: it specifies the quality of the astigmatism (regular or irregular), its axis, and detects surface or structural abnormalities that may limit the visual outcome.
Can dry eye disease affect the accuracy of topography?
Yes. An unstable tear film can make the maps less reliable and cause the astigmatism measurements to vary. This is why treatment of dry eye disease (artificial tears, eyelid hygiene, management of blepharitis) may be recommended before finalizing implant calculations. The goal is to obtain reproducible and consistent measurements from one session to the next.
Can topography help in choosing a toric implant?
Yes, it is in fact one of the key examinations. It precisely measures corneal astigmatism, its axis, and its regularity, which determines the indication for a toric implant and the correction strategy. It also helps verify the consistency between multiple measurements (biometry, refraction, keratometry) before deciding on the toric power.
Can I have a multifocal implant if I have astigmatism?
It depends on the type of astigmatism. Regular astigmatism can often be corrected (toric implant, combined strategy), which may make a multifocal or EDOF implant feasible in a well-selected patient. However, irregular astigmatism (irregular cornea, keratoconus, sequelae of surgery) makes multifocal implants riskier in terms of contrast and halos. In these cases, optical quality and comfort are generally prioritized.
After LASIK or PRK, is topography essential?
Yes, because the cornea has been reshaped and standard measurements may be less reliable if not interpreted correctly. Corneal topography (and often tomography depending on the device) helps verify regularity, detect any asymmetries, and guide the selection of appropriate calculation formulas for cataract surgery. The goal is to minimize the risk of refractive surprise and better plan the correction.
How long does a corneal topography examination take?
A few minutes. Image acquisition is very quick (often a few seconds per eye), painless, and non-contact. It may be necessary to repeat an acquisition if fixation was not optimal or if the ocular surface was too unstable (dryness, blinking).
📍 Consultation at Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan sees patients at the Paris – Auteuil Ophthalmology Practice for the diagnosis and surgical management of cataract surgery with corneal topography analysis. With a state-of-the-art technical platform including the latest OCT and biometry equipment, he offers personalized care adapted to each patient's situation.
Book an Appointment on Doctolib