
Myopic choroidal neovascularization is one of the most feared ocular complications in highly myopic patients. Dr Julien Gozlan, ophthalmic surgeon specializing in retinal diseases at the Paris – Auteuil Ophthalmology Practice, manages this macular condition using state-of-the-art diagnostic equipment including OCT and OCT angiography. This article details the pathophysiological mechanisms of myopic choroidal neovascularization, its symptoms, current diagnostic methods, treatment with anti-VEGF intravitreal injections, and long-term visual prognosis.
What is myopic choroidal neovascularization?
High myopia, or pathological myopia, is defined by an axial length exceeding 26 mm or a refractive error below -6 diopters. In these patients, progressive elongation of the eyeball causes mechanical stretching of the retina, choroid, and Bruch's membrane. When this membrane develops cracks (known as lacquer cracks or retinal stretch lines), it creates a breach that allows choroidal neovessels to proliferate beneath the retina. Myopic choroidal neovascularization, also called myopic choroidal neovascularization (myopic CNV), thus develops in the subretinal space, most commonly in a macular location, directly threatening central vision.
This complication affects approximately 5 to 11% of patients with high myopia. Unlike AMD, which occurs in elderly individuals, myopic choroidal neovascularization can appear in younger adults between 30 and 50 years of age, making it a particularly significant visual health concern. Myopic choroidal neovascularization is the leading cause of severe visual acuity loss in highly myopic individuals under 50 years of age.
Causes and risk factors of myopic choroidal neovascularization
The pathophysiology of myopic choroidal neovascularization involves several interrelated mechanisms:
- Mechanical stretching of the eyeball: progressive axial elongation weakens the posterior structures of the eye, particularly the choroid and Bruch's membrane.
- Bruch's membrane ruptures (lacquer cracks): these fissures serve as the entry point for neovessels that proliferate from the choriocapillaris into the subretinal space.
- Chorioretinal atrophy: progressive thinning of the choroid (often less than 50 µm on EDI-OCT) promotes local ischemia and the release of pro-angiogenic factors, notably Vascular Endothelial Growth Factor (VEGF).
- Posterior staphyloma: this deformation of the posterior pole worsens mechanical stress and promotes the development of myopic choroidal neovascularization.
- Genetic factors: a hereditary predisposition to pathological myopia increases the risk of neovascular complications.
The natural course without treatment is unfavorable: the neovascular membrane expands, causing subretinal hemorrhages, macular edema, and ultimately an irreversible fibrotic scar known as a Fuchs spot.
Symptoms and diagnosis of myopic choroidal neovascularization
Warning symptoms
Myopic choroidal neovascularization presents with symptoms that should prompt an urgent ophthalmology consultation:
- Sudden or rapidly progressive loss of visual acuity, especially in near vision.
- Metamorphopsia: distortion of straight lines, wavy perception of images, detectable using the Amsler grid test.
- Central scotoma: a dark or blurry spot in the center of the visual field.
- Micropsia: perception of objects as smaller than they actually are.
These symptoms, although common to other maculopathies such as macular hole or epiretinal membrane, must be addressed without delay in highly myopic patients.
Complete diagnostic workup
Diagnosis relies on a multimodal fundus examination:
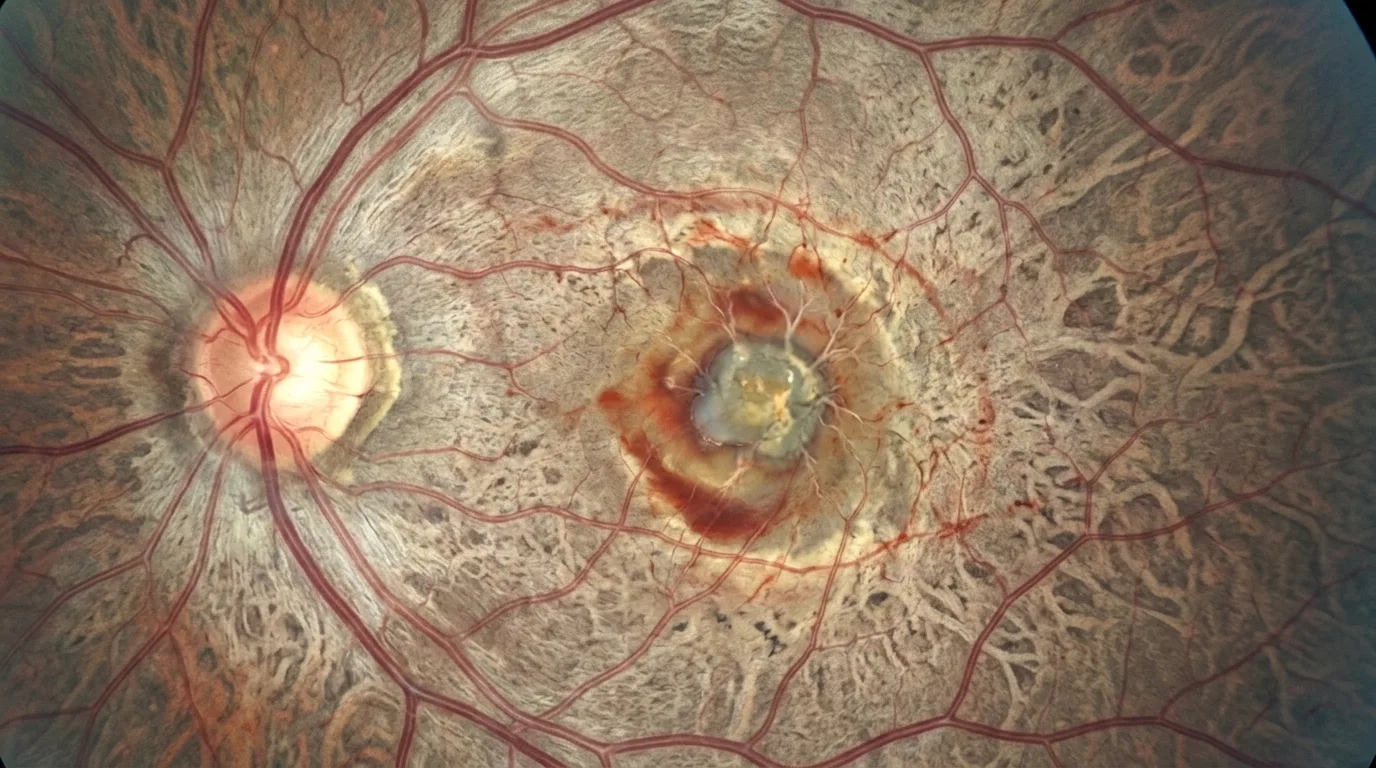
- Biomicroscopic fundus examination: visualization of a grayish or greenish lesion at the posterior pole, sometimes surrounded by a retinal hemorrhage.
- Macular OCT (optical coherence tomography): an essential examination that reveals a hyper-reflective thickening beneath the retinal pigment epithelium or in the subretinal space, a serous retinal detachment, and assessment of choroidal thickness using EDI (Enhanced Depth Imaging) mode.
- OCT angiography (OCTA): a non-invasive reference examination that allows direct visualization of the neovascular network without dye injection, with excellent sensitivity for detecting myopic choroidal neovascularization.
- Fluorescein angiography: reveals early hyperfluorescence with late leakage characteristic of active neovascularization.
- Indocyanine green angiography (ICG): useful for determining the extent and activity of the neovascular membrane, particularly in atypical cases.
Dr Julien Gozlan has a complete retinal imaging platform within his practice, enabling all of these examinations to be performed for accurate and rapid diagnosis of myopic choroidal neovascularization.
Treatment of myopic choroidal neovascularization with intravitreal injections
The standard treatment for myopic choroidal neovascularization relies on anti-VEGF intravitreal injections (IVT). This treatment has revolutionized the prognosis of this condition, which was previously responsible for legal blindness in many highly myopic patients.
Molecules used
Several anti-VEGF agents have demonstrated efficacy in the treatment of myopic choroidal neovascularization:
- Ranibizumab (Lucentis®): the first molecule to receive marketing authorization for this indication, validated by the RADIANCE study. Excellent results with a mean gain of +12 ETDRS letters at 12 months.
- Aflibercept (Eylea®): efficacy demonstrated in the MYRROR study, with a mean gain of +12 letters at 48 weeks. Approved for this indication.
- Brolucizumab (Beovu®) and faricimab (Vabysmo®): next-generation molecules currently being evaluated for use in myopic CNV.
Treatment protocol
Unlike exudative AMD, which often requires monthly injections, myopic choroidal neovascularization generally responds well to a lighter protocol:
- Loading phase: a single initial injection (unlike the 3 monthly injections for AMD), followed by reassessment at one month.
- Maintenance phase: PRN (pro re nata) strategy, meaning retreatment only in the event of recurrence documented by OCT and OCT angiography.
- Average number of injections: studies show that an average of 2 to 4 injections are needed in the first year, with fewer required in subsequent years.
This favorable response profile is explained by the typically smaller size of myopic choroidal neovascularization compared to that of AMD, and by a higher healing potential.
Visual prognosis and long-term follow-up
The visual prognosis for myopic choroidal neovascularization treated with anti-VEGF is generally favorable:
- Short term (1 year): 60 to 70% of patients gain at least 5 letters of visual acuity, and approximately 30 to 40% gain more than 15 letters.
- Medium term (2–3 years): visual gains are maintained in the majority of patients, with a decreasing number of injections.
- Long term (5 years and beyond): some patients develop progressive chorioretinal atrophy around the neovascular scar, which may secondarily limit the initial visual benefit. Regular follow-up therefore remains essential.
The most important prognostic factor is early diagnosis and treatment. Myopic choroidal neovascularization diagnosed early, before the development of extensive macular hemorrhage or fibrotic scarring, has a much better functional prognosis. Highly myopic patients should be educated about self-monitoring with the Amsler grid and should seek urgent consultation as soon as metamorphopsia appears.
Prevention and practical advice for highly myopic patients
Although there is no way to completely prevent myopic choroidal neovascularization, certain measures are recommended:
- Regular ophthalmological follow-up: annual assessment with macular OCT and dilated fundus examination for all patients with high myopia.
- Self-monitoring at home: daily use of the Amsler grid, one eye at a time, to detect metamorphopsia early.
- Emergency consultation: any change in central vision (decreased acuity, distortion, scotoma) should prompt an ophthalmology consultation within 48 hours.
- Sun protection: wearing UV-filtering lenses, although a direct link with neovascularization has not been formally established.
FAQ: myopic choroidal neovascularization
What is the difference between myopic choroidal neovascularization and that of AMD?
Myopic choroidal neovascularization occurs in younger patients (30–50 years) and results from Bruch's membrane cracks caused by globe elongation, whereas AMD-related neovascularization is linked to aging. Myopic neovascularization is usually smaller in size, which explains a better response rate to anti-VEGF therapy and often fewer injections. However, follow-up remains essential in both cases.
Is the intravitreal injection for treating myopic neovascularization painful?
Anti-VEGF intravitreal injection is performed under local anesthesia with eye drops. The procedure takes a few seconds and is usually very well tolerated. Patients may sometimes feel slight discomfort or a sensation of pressure, but rarely true pain. Mild ocular discomfort may persist for a few hours after the injection. Dr Julien Gozlan takes the time to explain each step to reassure his patients.
How many injections are needed to treat myopic choroidal neovascularization?
On average, 2 to 4 injections are needed in the first year, with a decreasing number in subsequent years. Unlike AMD, the protocol generally involves only a single initial injection, followed by retreatments guided by OCT. Some patients need only one or two injections in total, while others require more prolonged treatment in the event of recurrences.
Can good vision be recovered after myopic choroidal neovascularization?
Yes, the majority of patients treated early recover functional visual acuity. Clinical studies show a mean gain of 10 to 12 ETDRS letters at one year. The prognosis depends on the exact location of the neovascularization, its size, the speed of treatment, and the absence of pre-existing fibrotic scarring. Early diagnosis is the key factor in preserving vision.
What follow-up is needed after treatment of myopic choroidal neovascularization?
Follow-up is monthly during the first three months, then adjusted according to clinical progress and OCT results. During a stable phase, check-ups may be spaced to every two or three months. Long-term follow-up over several years is recommended, as late recurrences are possible. Self-monitoring with the Amsler grid complements this regular medical follow-up.
Can myopic choroidal neovascularization recur?
Yes, recurrences are possible and occur in approximately 30 to 40% of patients within the first two years. They may appear at the same site or at a different location on the macula. This is why regular follow-up with OCT and OCT angiography is essential to detect and treat any neovascular reactivation before it causes irreversible damage.
When should you consult Dr Julien Gozlan?
Any sudden vision loss, the appearance of metamorphopsia (distorted lines), a central scotoma, or a dark spot in the visual field in a highly myopic patient should prompt an urgent ophthalmology consultation to investigate myopic choroidal neovascularization. Patients with pathological myopia, even in the absence of symptoms, benefit from an annual assessment including macular OCT and fundus examination to detect any retinal complication early.
📍 Consultation at the Paris – Auteuil Ophthalmology Practice
Dr Julien Gozlan welcomes you at the Paris – Auteuil Ophthalmology Practice for the diagnosis and treatment of myopic choroidal neovascularization. With a complete retinal imaging platform (OCT, OCT angiography, angiography) and recognized expertise in medical retina, he offers you personalized, prompt, and reassuring care.
Book an Appointment on DoctolibFurther reading
- AMD: understanding age-related macular degeneration: causes, symptoms, and treatments of this maculopathy that shares common mechanisms with myopic neovascularization.
- Intravitreal injections (IVT): procedure, indications, and follow-up of anti-VEGF injections used in the treatment of choroidal neovascularization.
- OCT angiography: overview of this non-invasive examination essential for the diagnosis and monitoring of neovascular membranes.
- Macular OCT: how optical coherence tomography works and its value in the investigation of retinal diseases.